On June 3, 2026, the House Appropriations Full Committee passed the Fiscal Year (FY) 2027 appropriations bill for Interior, Environment, and Related Agencies, which was previously approved by the House Subcommittee on May 25, 2026. At the Subcommittee Hearing, Chairman Cole (R-OK-04), affirmed the Committee’s continued recognition and commitment to protecting the Indian Health Service (IHS) stating the bill “reflects our commitment to honoring and upholding our sacred trust and treaty oaths to protect Native American communities. I’m proud that the legislation prioritizes funding for the accounts that deliver critical services to Indian country.”
The bill provides $8.69 billion for IHS, including $6.06 billion in advance appropriations for FY 2028. The bill also expands advance appropriations to include Indian Health Facilities Sanitation Facilities Construction and Health Care Facilities Construction accounts. The bill authorizes $105.992 million for urban Indian health – an increase of $10.57 million over the FY26 enacted amount. The report states that “the Committee recognizes the Federal trust responsibility to provide health care services to American Indian and Alaska Native citizens and acknowledges that approximately seventy-one percent live in urban areas.”
Other key provisions include:
- $7 million for the Produce Prescription Pilot Program for Tribes and UIOs to increase access to produce and other traditional foods
- $45 million, a $5.57 million increase, for Tribal Epidemiology Centers (TECs).
Background
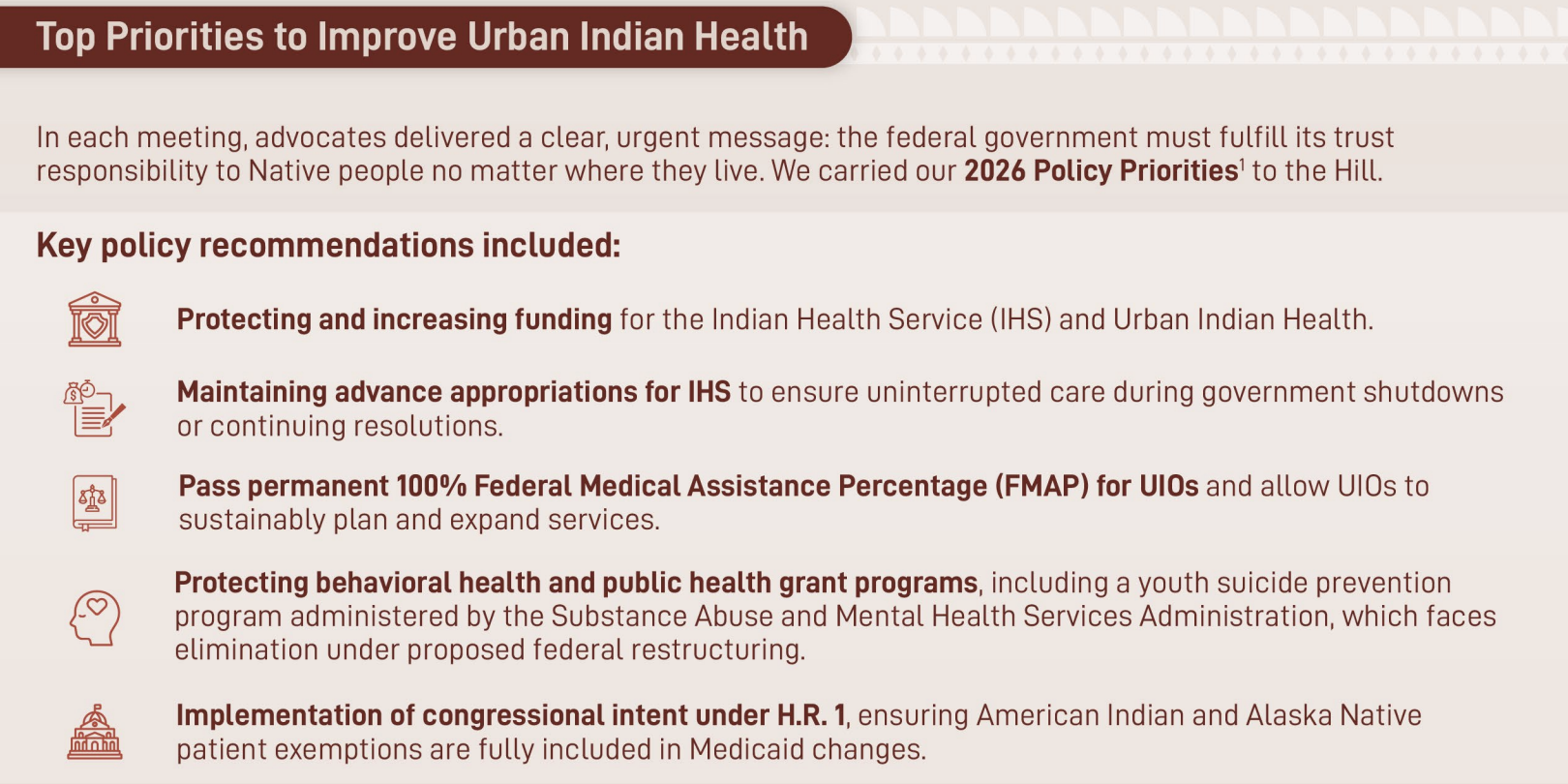
The National Council of Urban Indian Health (NCUIH) is a longstanding advocate for full funding for IHS and urban Indian health and supports the recommendations of the Tribal Budget Formation Workgroup. On March 17, 2026, NCUIH CEO Francys Crevier testified before the House Appropriations Subcommittee on Interior, Environment, and Related Agencies, urging full funding for urban Indian health and the Indian Health System.
NCUIH is also grateful for the support of Representatives working to support the health of Indian Country. On March 20, 2026, 59 Congressional leaders joined Representative Leger Fernandez in a bipartisan letter to Chairman Simpson and Ranking Member Pingree of the House Interior Appropriations Committee requesting support for Urban Indian Health, maintaining advance appropriations for IHS, and protecting IHS from sequestration. The letter emphasized that the federal government has a trust responsibility to provide federal health services to maintain and improve the health of American Indian and Alaska Native people.
Next Steps
The House will now need to schedule a floor vote on the Interior, Environment, and Related Agencies spending bill. The legislation is not expected to become law in its current form. House leadership will need to work with Senate Leadership to negotiate a final bill text for passage in both chambers.
FY26 funding is set to end on September 30, 2026. If Congress cannot come to a funding agreement by that deadline, they will need to pass a Continuing Resolution to keep the funding levels at the FY26 level until they reach an agreement. Should political disagreements lead to a government shutdown, UIOs and parts of IHS will be protected by Advance Appropriations.
Bill Highlights
| Line Item |
FY 26 Enacted |
FY 27 Tribal Request |
FY 27 President’s Budget |
FY 27 House Proposed |
| Urban Indian Health |
$95.42 million |
$1.09 billion |
$95 million |
$105.992 million |
| Indian Health Service |
$8.05 billion |
$73 billion |
$9.1 billion |
$8.69 billion |
| Hospital and Clinics |
$2.63 billion |
$18.5 billion |
$2.84 billion |
$2.87 billion |
| Tribal Epidemiology Centers |
$39.4 million |
____________ |
$39.4 million |
$45 million |
| Mental Health |
$133.69 million |
$5.41 billion |
$139 million |
$144.95 million |
Additional Key Provisions:
Clinical Decision Support for Diabetes Management (NEW)
Bill Report, Pg. 92,93: The Committee directs IHS to evaluate and, where clinically appropriate, implement evidence-based, artificial intelligence-enabled digital tools to improve insulin management, patient safety, and clinical outcomes in IHS facilities.
Rural Health Care Access (NEW)
Bill Report, Pg. 93: The Committee remains concerned about the ongoing difficulties rural and remote Tribal communities face in accessing timely health services. To reduce geographic barriers and improve care continuity, the Committee directs the IHS to procure integrated rural health care delivery models that leverage mobile medical units, telehealth-enabled clinical services, and clinical staff augmentation to address persistent workforce gaps.
IHS Hiring Initiative Follow Up (NEW)
Bill Report, Pg. 90: The Committee commends IHS on the launch of its fiscal year 2026 hiring initiative. As it works to streamline and expedite hiring processes, the Committee expects IHS to maintain the integrity and thoroughness of the background check process, and to consider ways to collaborate with and consult Tribes on hiring system improvements and decisions affecting healthcare services. The Committee encourages IHS to provide a report not later than 90 days following the enactment of this Act on its success in addressing the high staffing vacancy rate and implementing targeted recruitment and retention strategies in underserved areas.
Current Services: $264,752,000
Bill Report, Pg. 90: The Committee acknowledges that fixed costs continue to rise and flat funding results in a cut to programmatic dollars. The recommendation provides $264,752,000 for the Agency’s requested Current Services, which covers fixed costs for fiscal year 2027, for key health services to ensure increases go directly to programs. The Committee directs IHS to provide a detailed spend plan for fixed costs not later than 60 days following the enactment of this Act, including a timeline for when the funds will be distributed.
Produce Prescription Pilot Program: $7 million
Bill Report, Pg. 90: The recommendation includes $7,000,000 for IHS to expand, in coordination with Tribes and Urban Indian Organizations, the Produce Prescription Pilot to implement a produce prescription model to increase access to produce and other traditional foods among its service population. The Committee encourages IHS to provide a briefing not later than 90 days following the enactment of this Act on the distribution of funds and implementation efforts.
Contract Support Costs – $ 1.731 billion and Tribal 105(l) leases – $720 million
Bill Report, Pg. 93: The Committee recommends an indefinite appropriation estimated to be $1,731,000,000 for contract support costs incurred by the agency as required by law. The bill continues language making available such sums as are necessary to meet the Federal Government’s full legal obligation and prohibiting the transfer of funds to any other account for any other purpose. In addition, the bill includes language specifying carryover funds may be applied to subsequent years’ contract support costs.
Bill Report, Pg. 93: The Committee recommends an indefinite appropriation estimated to be $720,000,000 for Payments for Tribal Leases incurred by the agency as required by law. The bill includes language making available such sums as necessary to meet the Federal Government’s full legal obligation and prohibits the transfer of funds to any other account for any other purpose.
Purchased and Referred Care – $1.06 billion
Bill Report, Pg. 91: The recommendation includes $1,055,713,000 for Purchased and Referred Care (PRC). The amount provided reflects the fiscal year 2026 enacted base of $996,755,000, full funding for fiscal year 2027 current services requirements estimated at $45,958,000, and $13,000,000 for the purposes described below.
The Committee is aware that delayed reimbursements can cause financial strain on the Tribal member patient and the provider. This can sometimes result in the patient being incorrectly held liable for costs and cause medical debt to appear on the patient’s credit report. Therefore, within 90 days of the enactment of this Act, the Committee directs the Indian Health Service to report on ways to improve the speed at which reimbursement payments are paid to meet the 30-day requirement. The Committee also provides $13,000,000 for additional staff and resources needed to improve reimbursement timelines.
The Committee is interested in IHS findings on the Purchased and Referred Care funding distribution methodology and how PRC dependent areas, including those in California, are receiving the necessary PRC funds needed to purchase lifesaving care for Tribal members.
Indian Health Professions: $95,252,000
Bill Report, Pg. 92: The recommendation includes $95,252,000 for Indian Health Professions programs. The Committee continues to support Indian Health Professions programs and expects IHS to allocate the funding provided across all programs, including the Scholarship Program, Loan Repayment Program, Indians Into Medicine Program (INMED), American Indians into Nursing (RAIN) Program, and the American Indians into Psychology Programs.
The Committee appreciates the opportunities made available through Indian Health Professions programs like the Loan Repayment Program (LRP). The recommendation includes $53,000,000 for LRP to help offset student loan costs in exchange for two years of service at an Indian health program. The Committee remains concerned about the tax assessments associated with this grant program and the impact tax liabilities have on this valuable program. The Committee looks forward to the report from IHS and other applicable Bureaus and Agencies with respect to tax implications, as directed in House Report 119–215.
Sanitation Facilities Construction: $130,968,000
Bill Report, Pg. 94: The recommendation includes $130,968,000 for Sanitation Facilities Construction.
Health Care Facilities Construction: $190,508,000
Bill Report, Pg. 94: The recommendation includes $190,508,000 for Health Care Facilities Construction.
Equipment – Generators: $2.5 million in addition to FY26 amounts ($5 million)
Bill Report, Pg. 94: $2,500,000, in addition to amounts provided in fiscal year 2026, to purchase generators, including for IHS, Tribal Health Programs, and Urban Indian Organizations facilities located in areas impacted by de-energization events to increase the resilience of these facilities.
Dental Health: $287 million
Bill Report, Pg. 91: The recommendation includes $287,085,000 for Dental Health services.
- Also includes $1,500,000 to expand Dental Support Centers to all 12 service areas and $2,500,000 to install an electronic Dental Records System.
Alzheimer’s Disease: $6 million
Bill Report, Pg. 90: The recommendation includes $6,000,000 to continue Alzheimer’s and related dementia activities. These funds will enable awardees to continue to implement locally developed models of culturally appropriate screening, diagnostics, and management of people living with Alzheimer’s and other related dementia. This funding also supports the Dementia ECHO program, designed to support clinicians and caregivers to strengthen their knowledge and care around dementia for Tribal patients.
Improving Maternal Health: $3 million
Bill Report, Pg. 91: The recommendation also includes $3,000,000 for Improving Maternal Health. The Committee also recognizes the importance of in vitro diagnostics tools for the detection of diseases, infections, and other medical conditions. These tools provide valuable information to aid providers in accurate diagnostics, treatment planning, and monitoring of patient health. The Committee encourages the use of in vitro diagnostics in IHS health clinics and medical facilities.
Alcohol and Substance Abuse: $286 million
Bill Report, Pg. 91: The recommendation includes $286,389,000 for Alcohol and Substance Abuse programs.
Behavioral Health Pilot Program
Bill Report, Pg. 91: The Committee looks forward to the report on the status and outcomes of the new behavioral health pilot program that was enacted in fiscal year 2026 that supports grants to Indian Tribes, Tribal organizations, or consortia of Indian Tribes to operate and implement special behavioral health programs authorized by the Indian Health Care Improvement Act (25 U.S.C. 1665 et seq.) on or near an Indian Reservation.
Bureau of Indian Affairs, Missing and Murdered Indigenous Women Initiative: $33 million
Bill Report, Pg. 46: The recommendation includes $33,000,000 for the Missing and Murdered Indigenous Women Initiative to address the s women, including for criminal investigators, software platforms, and evidence recovery equipment. The Committee directs BIA to work with Tribal and Federal law enforcement agencies to facilitate sharing law enforcement and public records data and other technology.
NCUIH Contact:Meredith Raimondi, Vice President of Policy and Communications, mraimondi@ncuih.org