Senate Appropriations Committee Approves Labor-HHS Bill with Marginal Funding Increases for Indian Country
On July 27, 2023, the Senate Appropriations Committee approved the fiscal year (FY) 2024 Labor, Health and Human Services, Education, and Related Agencies appropriations bill with a vote of 26-2. The bill authorizes $117 billion for the Department of Health and Human Services (HHS)- a 6% decrease from the FY23 enacted level and $27.2 billion below the President’s Budget request. Other key provisions include an increase of $3,000,000 for National Health Service Corps (NHSC) Loan Repayment Program, and maintained funding for the Good Health and Wellness in Indian Country (GHWIC) program, the Tribal Behavioral Health Grants, and the American Indian/Alaska Native (AI/AN) set-aside funding for AI/AN Suicide Prevention Initiative. A more detailed analysis follows below.
NCUIH Advocacy
On March 23, 2023, NCUIH submitted written testimony to the Senate Committee on Appropriations, Subcommittee on Labor, Health and Human Services. The testimony outlined NCUIH priorities to fulfill the Tribal Budget Formulation Workgroup’s Budget Request for the Indian Health Service and the urban Indian line item, maintain advance appropriations for IHS, 100% Federal Medical Assistance Percentage (FMAP), increase funding for the electronic health record modernization, ensure UIOs are appropriately included in relevant grant programs, appropriate $80 million for the Native Behavioral Health Resources Program, as well as reauthorize the Special Diabetes Program for Indians.
Bill Highlights
Centers for Disease Control and Prevention (CDC) – Decrease of $20 million
- Bill Report, pg. 57: “The Committee recommendation provides a program level of $9,197,590,000 for the Centers for Disease Control and Prevention [CDC], which includes $55,358,000 in mandatory funds under the terms of the Energy Employees Occupational Illness Compensation Program Act [EEOICPA], and $1,186,200,000 in transfers from the Prevention and Public Health [PPH] Fund.”
Good Health and Wellness in Indian Country – Maintained funding
- Bill Report, pg. 69: “The Committee’s recommended level includes $24,000,000 for Good Health and Wellness in Indian Country.”
National Institutes of Health (NIH) – Increase of $943 million
- Bill Report, pg.88: “The Committee provides $49,224,000,000, an increase of $943,000,000, for the National Institutes of Health [NIH]”
Substance Abuse and Mental Health Services Administration
State Opioid Response Grants – Increase of $20 million
- Bill Report, pg. 149: “State Opioid Response [SOR] Grants: The Committee provides $1,595,000,000 for grants to States to address the opioid crisis. Bill language provides $60,000,000 for grants to Indian Tribes or Tribal organizations. The Committee supports the 15 percent set-aside for States with the highest age-adjusted mortality rate related to substance use disorders, as authorized in Public Law 117–328. Activities funded with this grant may include treatment, prevention, and recovery support services. States receiving these grants should ensure that comprehensive, effective, universal prevention, and recovery strategies are prioritized to account for comprehensive services to individuals”
- UIOs are not included
AI/AN Suicide Prevention Initiative – Maintained funding
- Tribal set-aside: $3.9 million
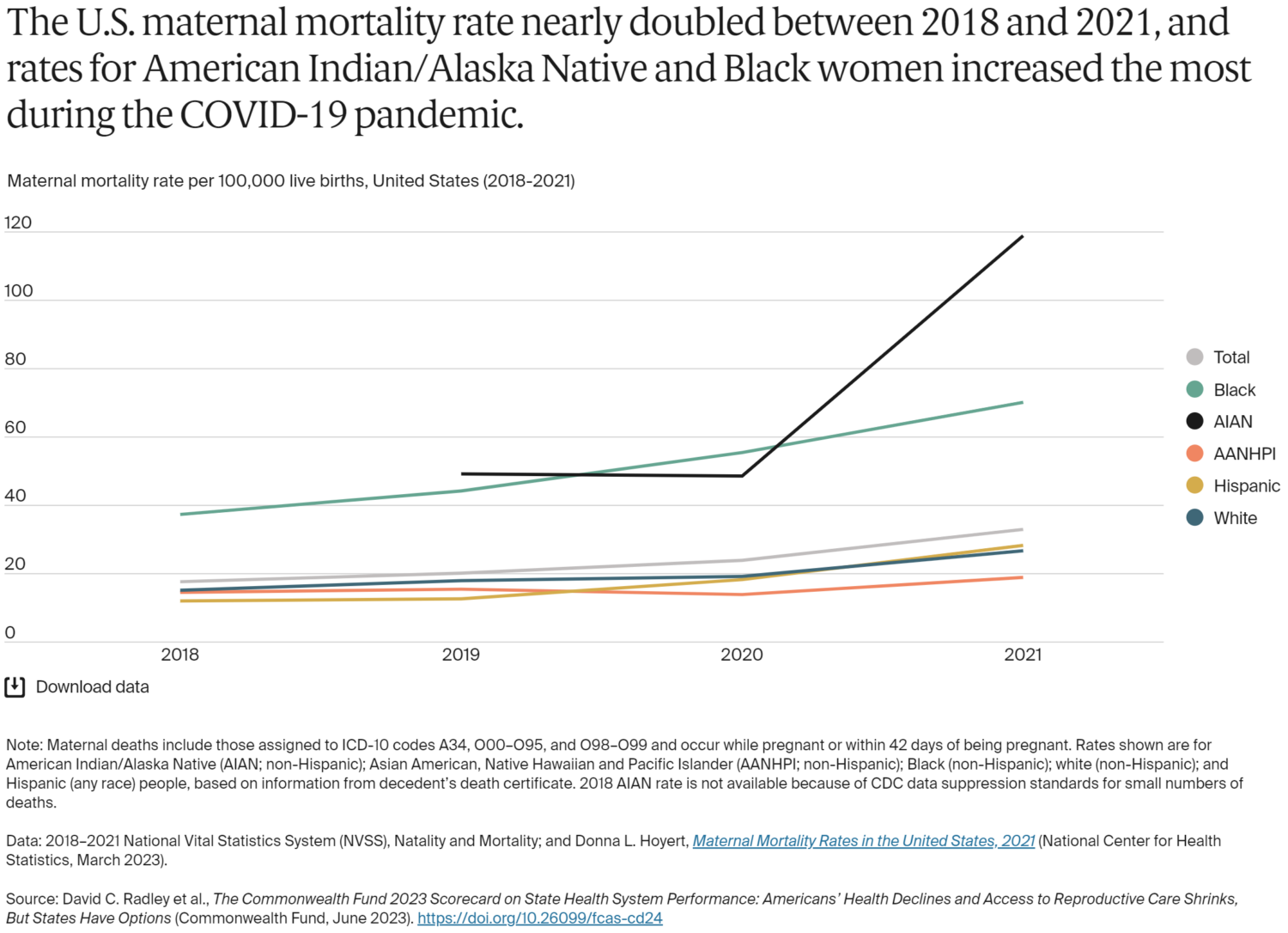
- Bill Report, pg. 142: “Suicide is often more prevalent in highly rural areas and among the American Indian and Alaskan Native populations. According to the CDC, American Indian/Alaska Natives [AI/AN] have the highest rates of suicide of any racial or ethnic group in the United States. In order to combat the rise in suicide rates among this population, the Committee recommends $3,931,000 for the AI/AN Suicide Prevention Initiative.”
Medication Assisted Treatment – Maintained funding
- Tribal set-aside: $14.5 million
- Bill Report, pg. 147, “The Committee includes $111,000,000 for medication-assisted treatment, of which $14,500,000 is for grants to Indian Tribes, Tribal organizations, or consortia.”
Tribal Behavioral Grants – Maintained funding
- Bill Report, pg. 152, “SAMHSA has administered Tribal Behavioral Health Grants for mental health and substance use prevention and treatment for Tribes and Tribal organizations since fiscal year 2014. In light of the continued growth of this program, as well as the urgent need among Tribal populations, the Committee continues to urge the Assistant Secretary for SAMHSA to engage with Tribes on ways to maximize participation in this program.”
- The bill provides $23,665,000 for the Tribal Behavioral Health Grants.
Health Resources and Services Administration (HRSA)
Community Health Centers – Maintained funding
- Bill Report, pg. 36, “The Committee provides $1,858,772,000 for the Bureau of Primary Health Care. Programs supported by this funding include community health centers, migrant health centers, healthcare for the homeless, school-based, and public housing health service grants. The Committee continues to support the ongoing effort to increase the number of people who have access to medical services at health centers. Health centers play a vital role in ensuring access to primary care in underserved areas of the country, including urban, rural, and frontier areas. In addition, within the amount provided, the Committee provides up to $120,000,000 under the Federal Tort Claims Act [FTCA] (Public Law 102–501 and Public Law 104–73), available until expended. These funds are used to pay judgments and settlements, occasional witness fees and expenses, and related administrative costs. The Committee intends FTCA coverage funded through this bill to be inclusive of all providers, activities, and services included within the health centers’ federally approved scope of project.”
National Health Service Corps – Increase of $3 million
- Bill Report, pg. 38, “The Committee provides $128,600,000 for the National Health Service Corps [Corps], an increase of $3,000,000 above the fiscal year 2023 enacted level. The Committee recognizes the success of the Corps program in building healthy communities in areas with limited access to care. The program has shown increases in retention of healthcare professionals located in underserved areas.”
Ending the HIV Epidemic – Maintained funding
- Bill Report, pg. 37, “The Committee provides $157,250,000 within the health centers program for the Ending the HIV Epidemic initiative. The initiative provides funding to Health Centers in high-need jurisdictions to increase prevention and treatment services for people at high risk for HIV transmission, including Pre-Exposure Prophylaxis [PrEP] related services, outreach, and care coordination through new grant awards in areas currently served by health centers.”
Native Hawaiian Health Care – Maintained funding
- Bill Report, pg. 37, “The Committee includes no less than $27,000,000 for the Native Hawaiian Health Care Program. Of the total amount appropriated for the Native Hawaiian Health Care Program, not less than $10,000,000 shall be provided to Papa Ola Lokahi for administrative purposes authorized under 42 U.S.C. 11706, including to coordinate and support healthcare service provision to Native Hawaiians and strengthen the capacity of the Native Hawaiian Health Care Systems to provide comprehensive health education and promotion, disease prevention services, traditional healing practices, and primary health services to Native Hawaiians.”
Center for Medicare and Medicaid Services
Tribal Health Care Reimbursements
- Bill Report, pg. 162, “The IHS rate does not reimburse Tribal healthcare providers for the cost of chemotherapeutics provided by a physician in the office setting. This makes the provision of cancer treatment on Indian reservations unsustainable for Medicare patients and damages the ability of American Indians to access local cancer treatment. The Committee urges CMS to clarify reimbursement procedures and amounts for Part B oncology drugs dispensed at IHS facilities to ensure parity among IHS and non-IHS facilities.”
Office of the Secretary
Center for Indigenous Innovation and Health Equity – Maintained funding
- Bill Report, pg. 203, “The Committee continues $4,000,000 to support the Center for Indigenous Innovation and Health Equity. The Committee recognizes the Center’s efforts to partner with institutions of higher education with a focus on Indigenous health research and policy among American Indians and Alaska Natives, as well as institutions of higher education with a focus on Indigenous health policy and innovation among Native Hawaiians/Pacific Islanders. The Committee encourages the Center to both continue and expand these efforts.”
National Cancer Institute
Alaska Native Colorectal Cancer
- Bill Report, pg. 89, “The Committee is concerned the Alaska Native people are twice as likely to be diagnosed with colorectal cancer as the White population. A recent study shows that Alaska Natives have the world’s highest rate of colorectal cancer. Colorectal cancer often has no symptoms until later stage, but screenings help detect growth at earlier stages. These high rates have led the Alaska Native Tribal Health Consortium and the Alaska Native Medical Center to amend their guidelines to lower the screening age from 45 to 40 in order to detect early-onset colorectal cancer. The Committee encourages NCI to expand research efforts to reduce Alaska Native cancer disparities and improve outreach.”
Climate and Health: Maintained Funding
- The Committee includes $10,000,000 for the program to provide guidance, data, and technical assistance to all States, local health departments, and additional assistance to Tribes and territories to identify possible health effects associated with a changing climate and implement health adaptation plans.