On March 28, 2022, President Biden released his Fiscal Year (FY) 2023 Budget. The budget includes $9.1 billion in mandatory funding for the Indian Health Service (IHS) for the first year, an increase of $2.9 billion above FY 2021, and $40.7 billion less than requested by the Tribal Budget Formulation Workgroup (TBFWG). The budget proposes increased funding for IHS each year over ten years, building to $36.7 billion in FY 2032, to keep pace with population growth, inflation, and healthcare costs. Funding for Contract Support Costs and 105(l) leases also shifted from discretionary to mandatory funding in the FY 2023 budget. The President’s budget does not include advance appropriations for IHS, which was requested in the FY 2022 budget. Note: The urban Indian health amount has not yet been released and detailed agency requests are expected to be available in the coming days.
Mandatory Funding for IHS
The Budget Brief stated, “The Administration is committed to implementing long-term solutions to address chronic under-funding of IHS and finally delivering on the nation’s promises to Indian Country.” Further, it states, “Implementing this change to the IHS budget will make meaningful progress toward redressing health inequities and ensuring that the disproportionate impacts of the COVID-19 pandemic on AI/AN communities are never repeated.” About the budget for IHS, President Biden stated it, “makes high-impact investments that will expand access to healthcare services, modernize aging facilities and information technology infrastructure, and address urgent health issues, including HIV and Hepatitis C, maternal mortality, and opioid use. It also includes funding to improve healthcare quality, enhance operational capacity, fully fund operational costs for Tribal health programs to support tribal self-determination, and recruit and retain healthcare providers.”
Advancing health equity by providing high quality care in Indian country is a priority for Biden. The budget book states, “Historical trauma and chronic underinvestment significantly contributed to the perpetuation of health disparities in Indian Country. These stark inequities illustrate the urgent need for investments to improve the health status and quality of life of AI/ANs. In FY 2023, the budget includes $6.3 billion in the Services account, an increase of $1.6 billion above FY 2022 enacted. These increases will expand access to programs that provide essential health services and community-based disease prevention and promotion in tribal communities. This funding will support additional direct patient care services across the IHS system, including inpatient, outpatient, ambulatory care, dental care, and medical support services, such as laboratory, pharmacy, nutrition, behavioral health services, and physical therapy.”
Chart from the Budget Book with Projected Funding for IHS
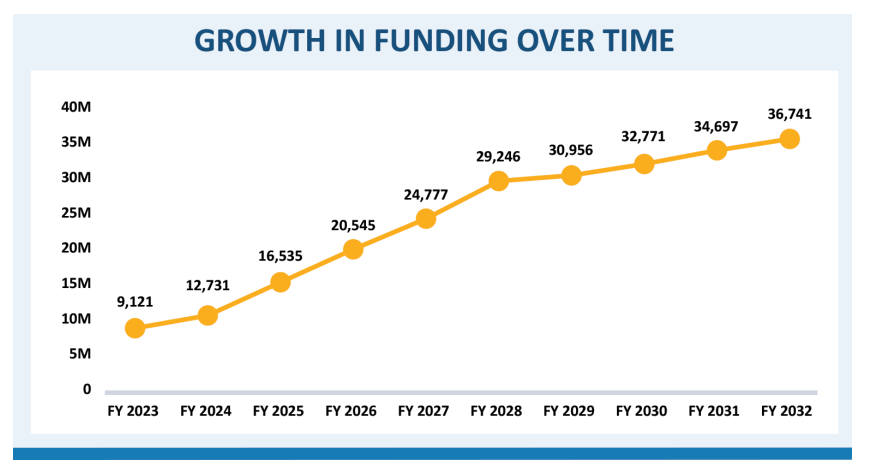
From President Biden’s Strengthening America’s Public Health Infrastructure section in the Budget, it states the following, “Guarantees Adequate and Stable Funding for the Indian Health Service (IHS). The Budget significantly increases IHS’s funding over time, and shifts it from discretionary to mandatory funding. For the first year of the proposal, the Budget includes $9.1 billion in mandatory funding, an increase of $2.9 billion above 2021. After that, IHS funding would automatically grow to keep pace with healthcare costs and population growth and gradually close longstanding service and facility shortfalls. Providing IHS stable and predictable funding would improve access to high quality healthcare, rectify historical underfunding of the Indian Health system, eliminate existing facilities backlogs, address health inequities, and modernize IHS’ electronic health record system. This proposal has been informed by consultations with tribal nations on the issue of IHS funding and will be refined based on ongoing consultation.”
Tribal Consultation Included as a Priority
According to the Budget, Tribal Consultation and Reconvening the White House Council on Native American Affairs was also included as priority. In his first days in office, the President issued a memorandum making it a priority of his Administration to make respect for Tribal sovereignty and self-governance, commitment to fulfilling Federal trust and treaty responsibilities to Tribal Nations, and regular, meaningful, and robust consultation with Tribal Nations cornerstones of Federal Indian policy. Since then, the Administration has been regularly meeting with Tribal Nations on a range of Administration priorities, from implementing the Bipartisan Infrastructure Law to drafting the President’s Budget.
Background and Next Steps
The Appropriations Committees will review the President’s Budget for consideration as they craft their bills for FY23. NCUIH has requested $949.9 million for FY23 for urban Indian health with at least $49.8 billion for the Indian Health Service in accordance with the Tribal Budget Formulation Workgroup (TBFWG) recommendations. NCUIH will continue to work with the Biden Administration and Congress to push for full funding of urban Indian health in FY 2023.
Overview of Budget Request
The budget request includes the following for American Indians/Alaska Natives:
Department of Health and Human Services (HHS)
- The Budget requests $127.3 billion in discretionary funding for HHS, a $26.9 billion or 26.8 percent increase from the 2021 enacted level.
Indian Health Service
- $9.1 billion in mandatory funding for the Indian Health Service (IHS) for the first year, an increase of $2.9 billion above FY 2021 and $40.7 billion less than requested by the TBFWG.
- Ending HIV and Hepatitis C in Indian Country ($52 million): Provides $47 million above FY 2022 enacted to enhance access to HIV testing, promote linkages to care, provide treatment, and reduce the spread of HIV 37 Indian Health Service Indian Health Service through the prescribing of pre-exposure prophylaxis (PrEP). Funds will also support enhanced surveillance and data infrastructure to better track HIV, Hepatitis C, and sexually transmitted diseases through Tribal Epidemiology Centers.
- Addressing Opioid Use ($20 million): Provides $9 million above FY 2022 enacted to enhance existing activities to provide prevention, treatment, and recovery services to address the impact of opioid use in AI/AN communities. This includes activities to increase knowledge and use of culturally appropriate interventions and encourage the use of medication-assisted treatment.
Maternal Health and Health Equity
- The United States has the highest maternal mortality rate among developed nations, and rates are disproportionately high for Black and American Indian and Alaska Native women. The Budget includes $470 million to: reduce maternal mortality and morbidity rates; expand maternal health initiatives in rural communities; implement implicit bias training for healthcare providers; create pregnancy medical home demonstration projects; and address the highest rates of perinatal health disparities, including by supporting the perinatal health workforce. The Budget also extends and increases funding for the Maternal, Infant, and Early Childhood Home Visiting program, which serves approximately 71,000 families at risk for poor maternal and child health outcomes each year, and is proven to reduce disparities in infant mortality. To address the lack of data on health disparities and further improve access to care, the Budget strengthens collection and evaluation of health equity data. Recognizing that maternal mental health conditions are the most common complications of pregnancy and childbirth, the Budget continues to support the maternal mental health hotline and the screening and treatment for maternal mental depression and related behavioral disorders.
- Improving Maternal Health ($10 million): Provides $4 million above FY 2022 enacted to improve maternal health in AI/AN communities. Funding supports preventive, perinatal, and postpartum care; addresses the needs of pregnant women with opioid or substance use disorder; and advances the quality of services provided to improve health outcomes and reduce maternal morbidity.
Department of the Interior (DOI)
- The Budget requests $17.5 billion in discretionary funding for DOI, a $2.8 billion or 19.3 percent
increase from the 2021 enacted level.
-
- $4.5 billion for the DOIs Tribal programs, a $1.1 billion increase above the 2021 enacted level.
- $632 million in Tribal Public Safety and Justice funding at DOI, which collaborates closely with the Department of Justice, including on continued efforts to address the crisis of Missing and Murdered Indigenous Persons.
Bureau of Indian Affairs (BIA)
- The Budget proposes to reclassify Contract Support Costs and Indian Self-Determination and Education Assistance Act of 1975 Section 105(l) leases as mandatory spending.
- Contract Support Costs: Contract Support Costs are the necessary and reasonable costs associated with administering the contracts and compacts through which tribes assume direct responsibility for IHS programs and services. These are costs for activities the tribe must carry out to ensure compliance with the contract but are normally not carried out by IHS in its direct operation of the program. The budget proposes to fully fund Contract Support Costs at an estimated $1.1 billion through an indefinite mandatory appropriation to support these costs in FY 2023. The indefinite mandatory appropriation grows with inflation and is maintained across the 10-year budget window to ensure Contract Support Costs continue to be fully funded each year.
- Tribal Leases: The Indian Self-Determination and Education Assistance Act requires compensation for reasonable operating costs associated with facilities leased or owned by tribes and tribal organizations to carry out health programs under the Act. In FY 2023, the budget proposes to fully fund section 105(l) leases, or tribal leases, at an estimated $150 million through an indefinite mandatory appropriation. The indefinite mandatory appropriation grows with inflation and is maintained across the 10-year budget window to ensure section 105(l) leases continue to be fully funded each year.
Bureau of Indian Education (BIE)
- $156 million increase to support construction work at seven Bureau of Indian Education schools, providing quality facilities for culturally appropriate education with high academic standards.
- $7 million for the Federal Boarding School Initiative.

