Urban Indian Organizations (UIOs) provide critical health care services to AI/AN people living in their service areas. UIOs play a vital role in upholding the federal trust responsibility that the United States (U.S.) Government holds with Tribes and American Indian/Alaska Native (AI/AN) people, as the large majority of AI/AN people live in urban areas. Currently, 41 UIOs are contracted with the Indian Health Service (IHS) under Title V of the Indian Health Care Improvement Act (IHCIA), representing 38 different urban areas within the U.S. These 41 UIOs consist of four different program types:
- Full ambulatory facilities (24)
- Limited ambulatory facilities (seven)
- Residential and inpatient treatment facilities (five)
- Outreach and referral facilities (five)
In 2025, the National Council of Urban Indian Health (NCUIH), reviewed all UIO services and programs provided as described on UIO websites, social media, and federal grant funding information databases. This overview of services demonstrates the wide range of multi-disciplinary programming that UIOs bring to their communities, with 80 percent of UIOs offering care for all four programming types: medical services, behavioral health services, social services, and traditional health practices.
Medical Services
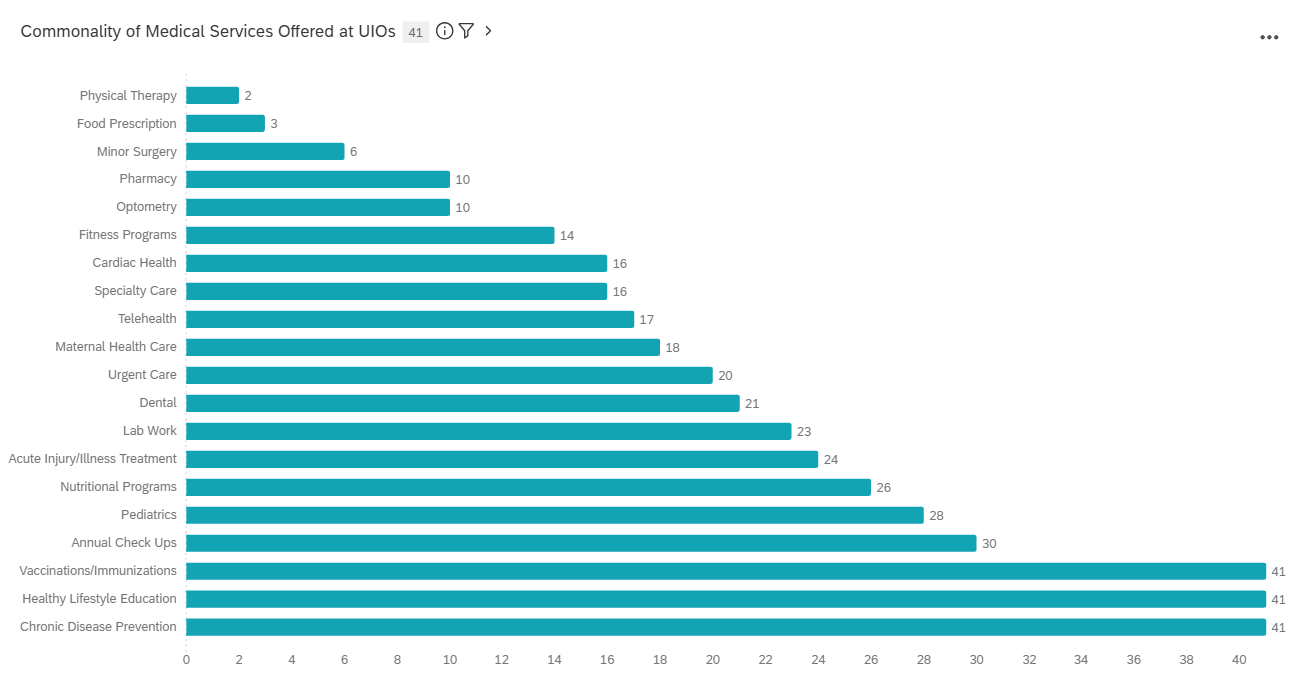
All UIOs offer immunizations, healthy lifestyle programming, and chronic disease prevention programming. Outside of those fundamentals, 85 percent of UIOs provide direct primary care services such as chronic disease management, regular physicals, urgent care, screenings, lab services, , and pregnancy and postpartum care. The Special Diabetes Program for Indians (SDPI) is at 78 percent of UIOs, an embodiment of the unique care that UIOs provide their patients that utilizes strengths within Indigenous communities to promote wellness while also managing existing chronic diseases like diabetes. SDPI allows for indigenized diabetes care, so programs not typically allowed from standard grant sources like Indigenous food cooking classes to help manage A1C levels, community gardens, traditional dancing classes for fitness, and culturally based youth groups all are incorporated into diabetes prevention and management programs. When programs are specifically tailored to the communities they serve and incorporate community and culture, this can increase participation and patient buy in (National Council of Urban Indian Health, 2024).
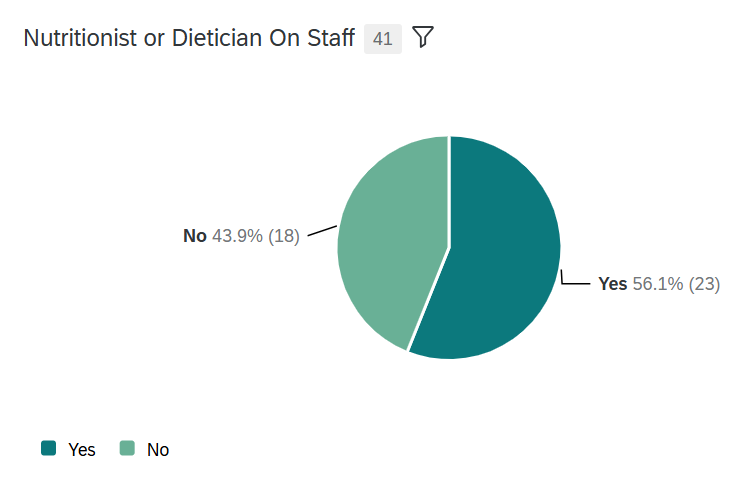
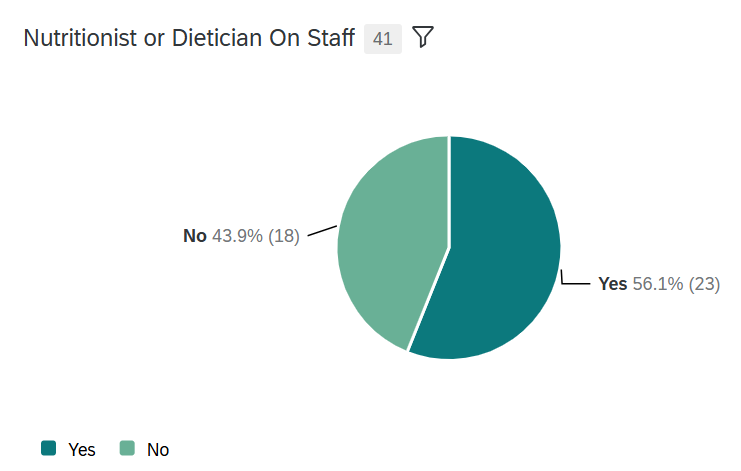
Some UIOs with advanced service providers provide specialty care for their patients with many sites offering services such as nutritionists/dietician visits, dental care, optometry, and minor surgeries in house. Several UIOs even include their own pharmacy, increasing accessibility and affordability for patients, which allows for supportive pharmacy-assisted chronic disease monitoring. Novel medical programs at UIOs include food prescription programs and mobile health vans increasing accessibility to care and promoting the inclusion of larger social drivers of health in healthcare programming.
Figure 1. Urban Indian organizations with a nutritionist or dietician on staff.
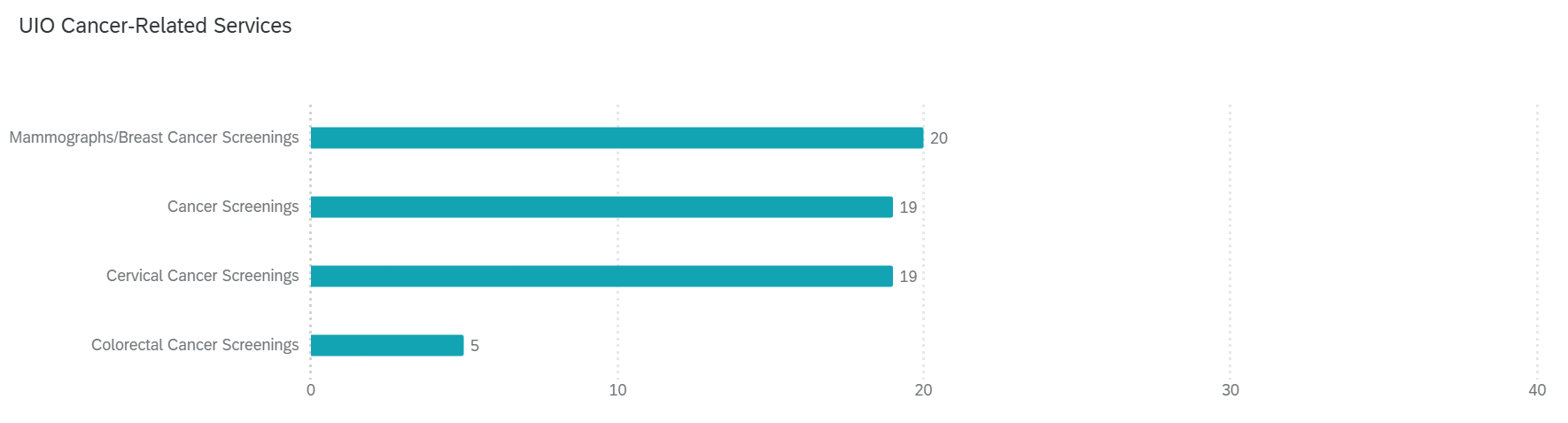
Interestingly, a little under half of UIOs provide cancer-related prevention services (49 percent) for their community members, which includes breast and cervical cancer screenings. An uncovered unmet need is in identifying colorectal cancer in urban AI/AN people, as the ability to test is only at 12 percent of UIOs. These services are less common because they are underfunded, not because they are not needed, and more funding and partnerships would bring more access to this area.
Figure 2. Urban Indian organizations’ cancer-related services offered
UIO providers emphasize the importance of their facilities offering care in house rather than referring out to ensure patient continuity of care, maintaining and strengthening patient relationships, and ensuring that care is culturally relevant for their patients. These medical services support all generations within these UIO communities bolstering much needed disease treatment and preventative care.
Figure 3. Commonality of medical services offered at urban Indian organizations
Behavioral Health Services
Behavioral health services are fundamental care at UIOs. All UIOs offer general counseling, with an emphasis on substance use disorders, and care for domestic violence/sexual assault victims. Counseling services vary in structure, with some offering family counseling, individualized counseling, and more. Other popular behavioral health services include consultation and assessment for diagnosis, support groups, intensive outpatient care, community education, and youth programs focused on promoting positive mental health practices for prevention.
Social Services
Figure 4. Urban Indian organizations with case workers or social workers available
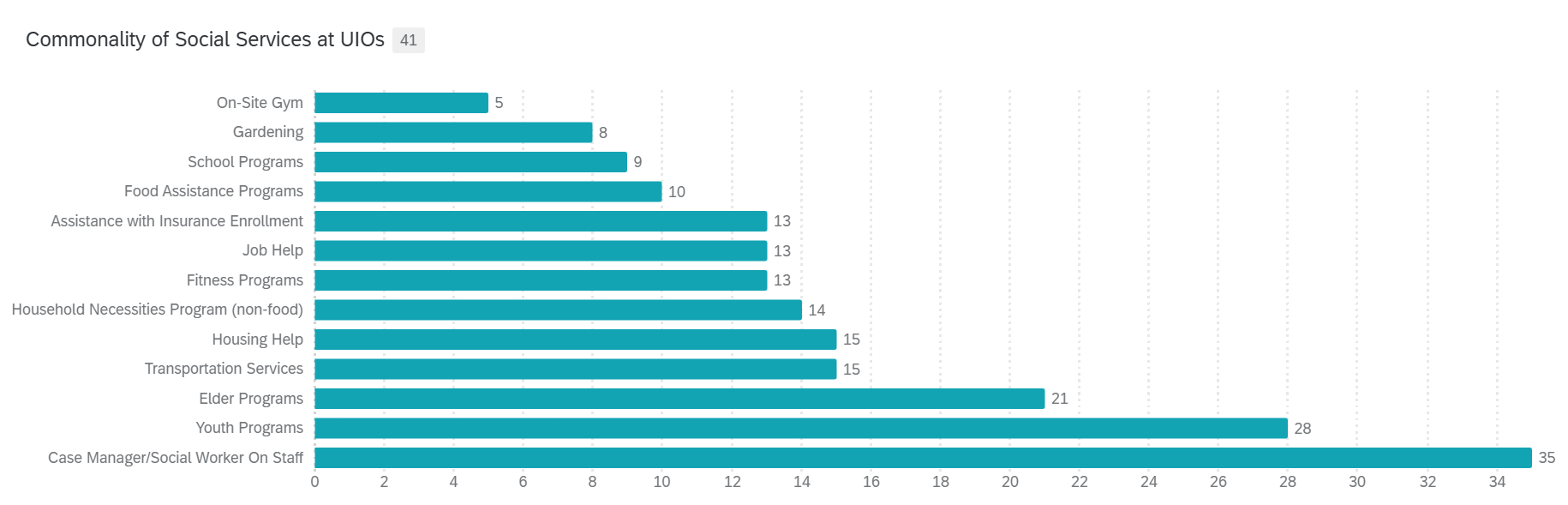
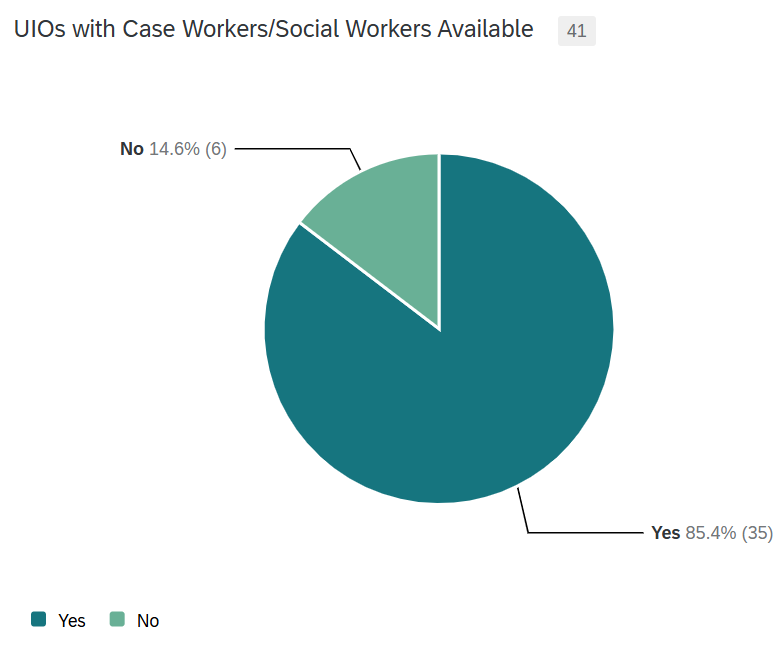 With a holistic approach to health, non-medical factors must also be addressed to provide the best care for patients. UIOs offer a variety of social services to ensure all the needs of their patients are met. This approach to care is exemplified by the 85 percent of UIOs that employ social workers or case workers for their patients. Other popular social services at UIOs include assistance with insurance enrollment, transportation to care, support with housing and other necessities, and elder programs. While not as common, a few UIOs are able to offer housing for their community, directly addressing the larger non-medical needs of their patients that impact health and wellness.
With a holistic approach to health, non-medical factors must also be addressed to provide the best care for patients. UIOs offer a variety of social services to ensure all the needs of their patients are met. This approach to care is exemplified by the 85 percent of UIOs that employ social workers or case workers for their patients. Other popular social services at UIOs include assistance with insurance enrollment, transportation to care, support with housing and other necessities, and elder programs. While not as common, a few UIOs are able to offer housing for their community, directly addressing the larger non-medical needs of their patients that impact health and wellness.
Figure 5. Commonality of social services offered at urban Indian organizations
Traditional Healing
UIOs are set apart from standard health organizations as seen through the culturally relevant care they provide to their community. Many Urban Native people are unable to participate in traditional healing or ceremony due to living away from their Tribal communities, but almost all UIOs (95 percent) offer different ways to reconnect their patients with Traditional Healing as part of their programming. This programming highlights the significance of UIOs within their communities, providing culturally relevant care that is grounded in Indigenous concepts and practices of wellness. Talking circles are the most common traditional practice, with 61 percent of UIOs offering this practice. Traditional healing-based substance use treatment programs (i.e. Wellbriety), traditional drumming, traditional medicines, traditional arts, and Indigenous foods are also common traditional healing-based programs and practices that UIOs provide for their patients.
As shared by UIO staff in NCUIH’s 2023 report, traditional healing is in high demand within UIO communities (National Council of Urban Indian Health, 2023b). It offers a mechanism to combat social isolation, strengthen community and cultural connection, and promote wellness (National Council of Urban Indian Health, 2023b). However, many of these programs, as well as standard health services, are underfunded at UIOs, making it difficult for UIOs to fully meet the needs of the communities they serve (National Council of Urban Indian Health, 2023b).
Funding
It is vital that UIOs receive stable and sustained funding for their work to maintain their work in promoting healthier communities and providing life-saving care. Outside of IHS, Medicaid and the Children’s Health Insurance Program (CHIP) are the largest sources of funding for UIOs (National Council of Urban Indian Health, 2023a). Medicaid and CHIP reimbursement supplement the chronically low congressional appropriations to UIOs. Increased ability for Centers for Medicare & Medicaid Services (CMS) to reimburse for UIO services, like applying 100 percent federal medical assistance (FMAP) percentage would better support the work UIOs do to combat health disparities.
Many UIO programs and services are also funded through grants, but sustainability and relevance of grant opportunities do not always match the needs of AI/AN communities. Grants should adapt to better suit the Native communities they wish to support by extending grant life cycles, allowing funding for cultural activities and priorities, and increasing focus on preventative health programming (National Council of Urban Indian Health, 2023b).
UIO leaders outlined their priorities for 2026 with NCUIH with the top items emphasizing funding:
- increasing congressional funding for Urban Indian Health
- securing 100 percent federal medical assistance percentage (FMAP)
- increasing general behavioral health funding (National Council of Urban Indian Health, 2025)
Despite the limited funding allocated to them, UIOs are integral parts of the AI/AN communities they serve and do much with the fraction of need provided. With more AI/AN people living away from Tribal lands, and thus Tribal health and IHS facilities, it is necessary that funding for AI/AN healthcare reflects the need for greater urban funding to uphold the trust responsibility to urban AI/AN people. By embracing an Indigenous holistic approach to care, UIOs uplift Urban AI/AN people when they most need it.
To cite information about UIO services and programming as detailed in this blog post, please use the following citation:
National Council of Urban Indian Health (2026). Urban Indian Organizations’ Programming Profile.
Citations:
National Council of Urban Indian Health. (2023a). An Overview of the Impact of Medicaid on Health Care for American Indians and Alaska Natives. https://ncuih.org/wp-content/uploads/Impact-Medicaid_NCUIH_D329_F2.pdf
National Council of Urban Indian Health. (2023b). (rep.). Recent Trends in Third Party Billing: Thematic Analysis of Traditional Healing Programs at Urban Indian Organizations and Meta-Analysis of Health Outcomes. Retrieved from https://ncuih.org/wp-content/uploads/03.25.24-FINAL-design-of-2023-TH-Report.pdf.
National Council of Urban Indian Health. (2024). (rep.). Recent Trends in Third Party Billing: Thematic Analysis of Traditional Food Programs at Urban Indian Organizations and Research on Traditional Healing. Retrieved 2026, from https://ncuih.org/wp-content/uploads/Traditional-Food-Report-NCUIH-D507_F2.pdf.
National Council of Urban Indian Health. (2025, November). Summary of NCUIH Policy Priorities Survey for 2026.