March Policy Updates: Key Policy Changes, Funding News, and Upcoming Events
🤝 Register for NCUIH’s 2025 Conference and Hill Day!
🆕 New Resource: NCUIH releases new resource highlighting Medicaid’s crucial role for Native communities.
🚨 Proposed Medicaid Changes – NCUIH works with partners to support Medicaid and Children’s Health Insurance Program (CHIP).
📜 Legislative Updates – Senate Committee on Indian Affairs (SCIA) advances NCUIH-endorsed legislation impacting Native communities.
🏛 Appropriations Updates – Status of Continuing Resolution and Fiscal Year (FY) 2025 Funding.
⚖ Lawsuits & Court Cases Updates – Current court cases and legal action impacting Native health care and policy.
📬 Federal Agency Notices and Comment Opportunities – U.S. Department of Housing & Urban Development (HUD) releases advisory opinion on application of DEI executive orders, Executive Order 14112 rescinded, Department of Health and Human Services (HHS) releases revised notice and comment policy, and Government Accountability Office continues to list the Indian Health Service (IHS) on high-risk list.
🎤 NCUIH in Action – NCUIH joins federal agency tribal advisory groups in key discussions impacting Native communities.
📜 Tribal Coalition Update – A coalition of 20+ Tribal organizations mobilizes to protect IHS and Native health programs from administrative threats.
📆 Upcoming Events – Tribal Self-Governance Conference, HHS FY 2027 Annual Tribal Budget Consultation, and Federal Tribal Advisory Committees.
Register for NCUIH’s 2025 Conference and Hill Day!

Join us for Hill Day!
We invite you to participate in Hill Day on Friday, April 25, 2025, in Washington, D.C. This is an opportunity to meet with congressional offices, share the impact of Urban Indian Organizations (UIOs), and highlight the importance of policies that support urban Indian health.
To join us, please complete the participation form by Monday, April 7, 2025.
Call for Nominations!
As part of our commitment to uplifting excellence in health care, we are seeking nominations for individuals and organizations who have made remarkable contributions to the field of urban Indian health.
Please submit your nominations using this form, which includes detailed instructions on the nomination process and criteria for each award. The deadline for submissions is Friday, March 28, 2025.
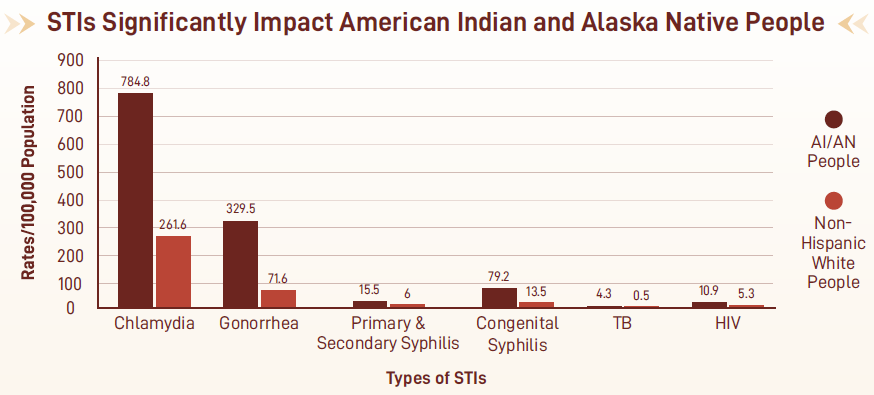
NCUIH Releases New Resource Highlighting Medicaid’s Crucial Role for American Indian and Alaska Native Communities
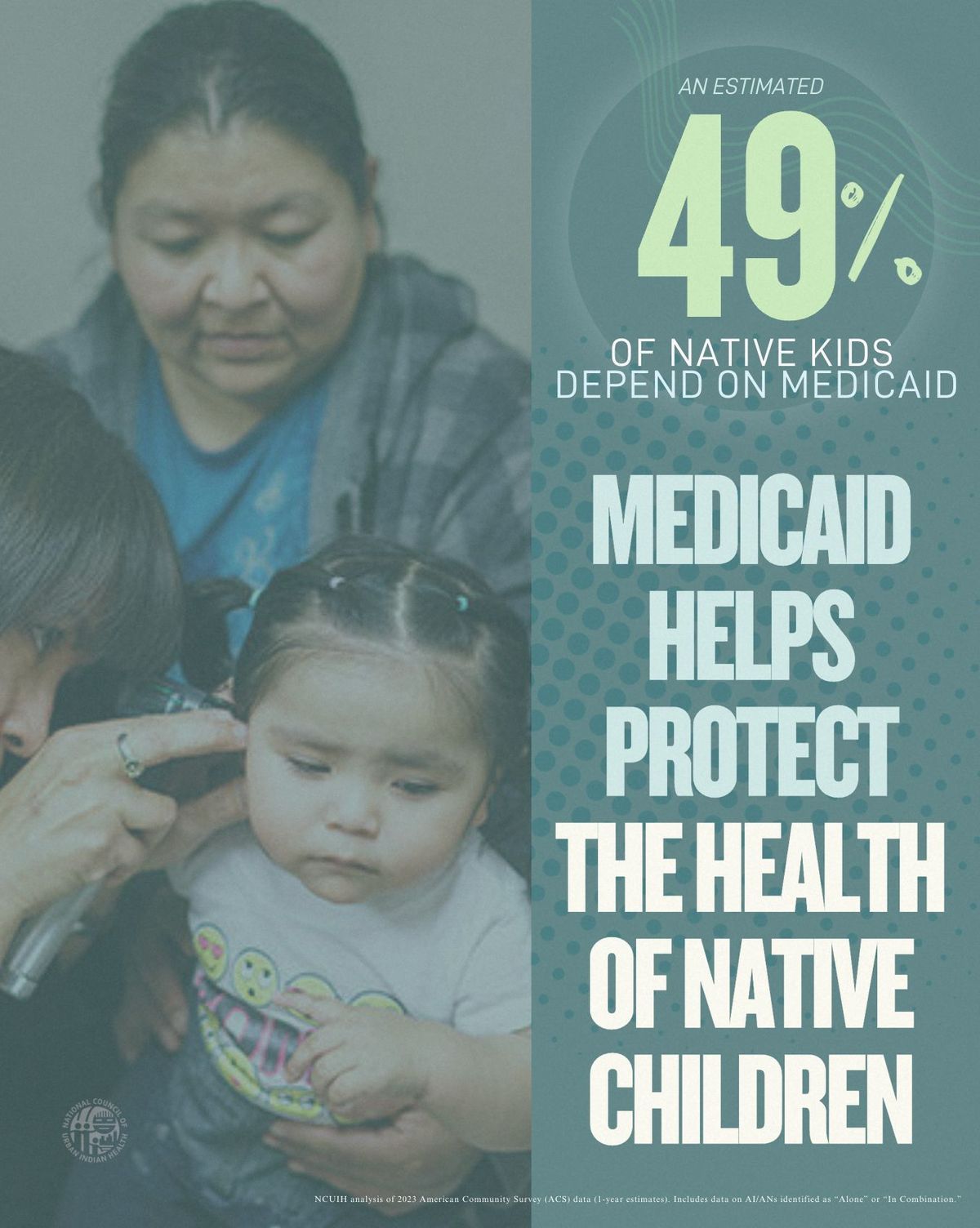
NCUIH has released a comprehensive overview highlighting the crucial role Medicaid plays in providing health care to Native communities. This report emphasizes the importance of preserving Medicaid resources and exempting Native beneficiaries from work requirements to fulfill the federal government’s trust responsibility.
By the numbers:
- Approximately 2.7 million Native people are enrolled in Medicaid, with 24% of Native adults aged 18-64 and 23% of those over 64 benefiting from the program.
- Almost 49% of Native children are enrolled in Medicaid.
- UIOs serve as vital health care providers.
- 59% of Native people receiving care at UIOs are Medicaid beneficiaries.
- Eight out of the top ten states with the largest number of Native Medicaid beneficiaries have UIOs providing essential services
Read more on our blog.
NCUIH Joins Coalition in Urging Bipartisan Support for Medicaid and CHIP Programs
On March 3, NCUIH joined 30 national and state level provider groups, health plan associations, other groups in signing on to the Medicaid Health Plans of America (MHPA) letter to the Chairs and Rankings Members of the Senate Finance and House Energy & Commerce Committees, expressing strong support for the importance of Medicaid and CHIP.
- Why it Matters: In 2023, approximately 2.7 million Native people were enrolled in Medicaid across the United States, according to American Community Service data. Medicaid is a major source of health care funding, particularly for UIOs, which provide essential healthcare services to Native people living in urban areas. The letter emphasizes the importance of Medicaid and CHIP as a source of funding for critical safety net facilities and encourages Congressional leadership to continue in a tradition of bipartisan support for these vital programs.
- Read more on our blog.
NCUIH continues to collaborate with partners to protect essential funding for Medicaid and CHIP.
Senate Committee on Indian Affairs Advances NCUIH-Endorsed Legislation Impacting Native Communities
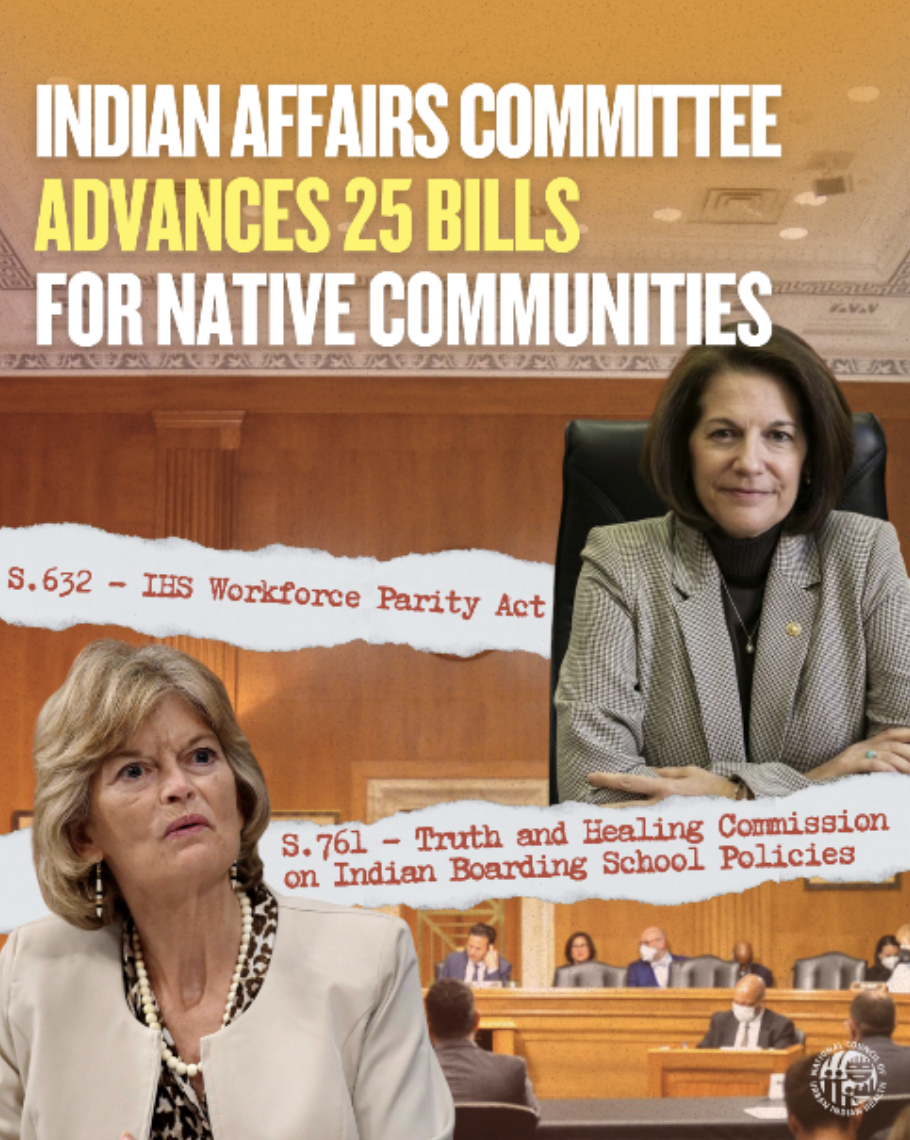
On March 6, the Senate Committee on Indian Affairs (SCIA) advanced 25 bills impacting Native communities. Among them were three NCUIH-endorsed bills: the Truth and Healing Commission on Indian Boarding School Policies Act of 2025 (S.761), the Bridging Agency Data Gaps and Ensuring Safety (BADGES) for Native Communities Act (S.390), and the IHS Workforce Parity Act (S.632).
S. 632 – IHS Workforce Parity Act
- This legislation amends the Indian Health Care Improvement Act to allow Indian Health Service scholarship and loan recipients (including those work at UIOs) to fulfill service obligations through half-time clinical practice
S. 761 – Truth & Healing Commission on Boarding Schools
- This legislation establishes a formal commission to investigate, document, and acknowledge past injustices of the federal government’s Indian Boarding School Policies.
S.390 – BADGES for Native Communities Act
- This bill requires law enforcement agencies to report on cases of missing or murdered Native people.
- UIOs are eligible entities for the missing or murdered response coordination grant program, established by the bill, allowing UIOs to create and grow programs to assist in developing coordinated responses and investigations for MMIP.
Next Steps: The bills have been advanced to the full Senate for consideration, and NCUIH will continue to closely monitor their progress.
Read more on our blog.
Continuing Resolution and FY 2025 Funding

On March 14, 2025, The House and Senate passed a Continuing Resolution (CR) to extend government funding set to expire on March 14, 2025, until September 30, 2025.
Key Provisions:
- Maintains advance appropriations for IHS.
- Extends funding for the Special Diabetes Program for Indians (SDPI). Brings total FY25 funding to $159,422,727.
- Extends Medicare Telehealth Flexibilities
NOTE: Our Policy Alert sent out on March 14, 2025, stated that the CR eliminated funding for FY24 earmarked projects. Further analysis shows that the CR simply prevents the FY24 projects from being funded twice and does not rescind any funding appropriated for such projects in the original FY24 appropriations bill.
Read more on our blog.
Monitoring The Bench: Lawsuits Filed Against Recent Executive Orders and Presidential Actions

State of New York v. Trump – A lawsuit filed in the District Court of Rhode Island by 22 states to stop the federal funding freeze.
- The court issued a Preliminary Injunction on March 6, 2025, preventing the federal government from pausing, freezing, canceling, or impeding the disbursement of appropriated federal funds.
- The defendants filed an appeal on March 10 with the First Circuit.
National Council of Nonprofits v. Office of Management and Budget (OMB) – A lawsuit filed in the District Court of the District of Columbia by nonprofits challenging the federal funding freeze.
- The court granted a preliminary injunction on February 25, 2025, blocking the government from freezing or rescinding any appropriated funds nationwide.
Pueblo of Isleta v. Secretary of the Department of the Interior – A lawsuit filed on March 7, 2025, in the District Court for the District of Columbia by Tribes impacted by the Bureau of Indian Education (BIE) reorganization and staff reductions.
- The lawsuit claims BIE failed to consult Tribes before implementing these changes, which have affected student services and school maintenance.
Over 100 lawsuits have been filed against recent executive orders and presidential actions, covering issues like agency data access, federal employee terminations, and elimination of diversity, equity, and inclusion (DEI) initiatives. NCUIH continues tracking these cases to identify any rulings that may impact UIOs.
HUD Memo on Application of DEI Executive Orders
On March 13, the United States Department of Housing and Urban Development (HUD) General Counsel issued a memorandum on application of DEI executive orders.
- This memorandum states that the Executive Orders on DEI do not apply to HUD’s legal obligation to provide housing for Indian Tribes and their citizens.
- The Executive Orders on DEI also do not apply to the government-to-government relationship that underlies those obligations.
Executive Order 14112 Rescinded
On March 14th, President Trump Rescinded Executive Order 14112 of December 6, 2023 (Reforming Federal Funding and Support for Tribal Nations to Better Embrace Our Trust Responsibilities and Promote the Next Era of Tribal Self-Determination).
- On March 14, President Trump signed an Executive Order entitled “Additional Rescissions of Harmful Executive Orders and Actions.” Section 2(p) rescinds Executive Order 14112 of December 6, 2023.
- NCUIH is analyzing this impact on UIOs.
NCUIH remains committed to upholding the federal trust responsibility for Native healthcare.
HHS Revised Notice and Comment Policy & Upcoming Federal Agency Comment Opportunities
HHS Revised Notice & Comment Policy: HHS has updated procedures on how Tribal and Urban Indian input is solicited.
On March 3, HHS announced in a policy statement that HHS is rescinding a 1971 statement of policy that waived Administrative Procedure Act (APA) exemptions for rules and regulations relating to public property, loans, grants, benefits, or contracts.
- HHS states that HHS will continue to follow notice and comment rulemaking procedures in all instances in which it is required to do so by the statutory text of the APA.
- HHS and IHS both have Tribal Consultation policies and IHS’ has an Urban Confer policy. Thus, even if HHS may not provide a notice and comment period in the Federal Register, if the matter concerns Tribes, a Tribal Consultation may be required per HHS and IHS policies or an Urban Confer may be required per IHS policy if UIOs are implicated.
- However, for activities outside of IHS, an Urban Confer may not be required because HHS does not have an Urban Confer Requirement. There may also be instances where engagement may not be required even if Tribal and/or UIO interests are impacted.
Upcoming Federal Agency Comment Opportunities:
Apr. 21 – HHS 27th Annual Tribal Budget Consultation (ATBC)
- The 27th HHS ATBC will be on April 22-23, 2025, at HHS. The ATBC will provide a forum for Tribes to collectively share their views and priorities with HHS officials on national health and human services funding priorities and make recommendations for the Department’s FY 2027 budget request.
- Comment Deadline: The written comment period is open until April 21, 2025, at 5 p.m. EDT to consultation@hhs.gov.
ICYMI: Recent Dear Tribal and Urban Leader Letters (DTLL/DULL)

Recent Dear Tribal and Urban Leader Letters (DTLL/DULL)
March 6 DTLL – IHS Process for Requesting a Tribal Delegation Meeting with IHS Director
- The IHS Acting Director writes to Tribal Leaders to share updates on enhancements to the process for requesting a Tribal Delegation Meeting (TDM) with the IHS Director.
- Direct all TDM requests IHSTribalDelegationMeeting@ihs.gov
- All TDMs will be scheduled by the IHS TDM Coordinator no sooner than 2 weeks after a TDM request is received.
- The IHS is also inviting Tribal Leaders to contribute to a display honoring Tribal Nations that will be installed at IHS Headquarters.
United States Government Accountability Office Continues to List IHS on High-Risk List
On February 25, 2025, the United States Government Accountability Office (GAO) updated GAO’s “High Risk List” by adding a new area on federal disaster assistance and released the report “Heightened Attention Could Save Billions More an Improve Government Efficiency and Effectiveness.”
- GAO continues to list “Improving Federal Management of Program that Serve Tribes and Their Members” – including IHS- on the High-Risk List.
- GAO states that IHS has met one criterion for removal from the High-Risk List- “Leadership Commitment”- but the four other criteria- “Capacity,” “Action Plan,” “Monitoring,” and “Demonstrated Progress”- are partially met and still need attention.
NCUIH will continue to monitor for any developments. Read more on our blog.
UIOs at the Joint Session of Congress

Two Native health leaders were invited to attend the Joint Session of Congress in Washington, D.C. on March 4. Dr. Linda Son-Stone, CEO of First Nations Community HealthSource, attended as a guest of Congresswoman Melanie Stansbury (NM-01). Walter Murillo, CEO of Native Health Phoenix and NCUIH Board President, attended as a guest of Congressman Greg Stanton (AZ-04). Both Stansbury and Stanton are members of the Native American Caucus.
The Joint Session of Congress presents an opportunity to emphasize the importance of honoring the federal trust responsibility to provide adequate healthcare to Native people. Both leaders have dedicated their careers to advocating for the health and well-being of urban Native populations. Their invitations are a recognition of the key role of UIOs in providing healthcare to Native communities.
Read NCUIH’s press release here.
NCUIH in Action

HHS Secretary Robert R. Kennedy Jr. and NCUIH CEO Francys Crevier (Algonquin) at the HHS Secretary Tribal Advisory Committee on February 26.
NCUIH Joins Federal Agency Tribal Advisory Groups in Key Discussions Impacting Native Communities
February 25-26: HHS Secretary Tribal Advisory Committee (STAC)
What they are saying:
- HHS announced the establishment of the Make American Healthy Again Commission – Chaired by Secretary Kennedy.
- Assistant Secretary for Financial Resources noted that IHS will not face sequestration with a new CR.
- Health Resources and Services Administration encouraged urban Indian health clinics to apply for the National Maternal Health Mental Health Hotline and the National Health Service Loan Repayment Program.
- Center for Medicaid and CHIP Services acknowledged that Medicaid resources for IHS, Tribal, and urban Indian health programs are critical.
- Substance Abuse and Mental Health Services Administration (SAMHSA) shared that SAMHSA continues to prioritize Tribes and Tribal organization for funding and anticipates more funding in FY25.
- IHS noted that it is getting back into core duties and IHS priorities and strategic goals have not changed.
- During the meeting, Secretary Kennedy offered protections to Tribal leaders and the Indian health system, stating, “When they announced $9.6 billion in cuts to my agency—10% of our workforce—the one sub-agency I insisted must be protected was IHS. We safeguarded 1,000 jobs at IHS, and we will continue to do so. As new orders and additional cuts come down, protecting these jobs remains my priority.”
- Did you know?: On March 12, NCUIH sent a letter to HHS requesting that Secretary Kennedy intervene to exempt IHS from workforce reductions and hiring freezes and protect IHS funding from sequestration and impoundment.
February 25-26: Department of Veterans Affairs (VA) Advisory Committee on Tribal and Indian Affairs
What they are saying:
- The Office of Urban Indian Health Programs noted a key change in the proposed IHS reorganization includes the creation of a dedicated VA office within IHS to focus solely on VA partnerships.
- While the reorganization is progressing, implementation has been delayed, especially due to a hiring freeze preventing the appointment of a director.
- VA Office of Tribal Health (OTH) spoke about the “Clinic in a Clinic” program.
- This is a program that combines VHA and IHS to allow VHA providers to work at Indian health facilities to provide care directly to Native patients.
- There are currently two Clinic in a Clinic programs on the Navajo Nation. OTH is looking to expand this program to more clinics, and it can be implemented at any IHS, Tribal Program, or UIO facility.

HHS Secretary Robert R. Kennedy Jr. and NCUIH CEO Francys Crevier (Algonquin) at the HHS Secretary Tribal Advisory Committee on February 26.
March 26-27: CMS Tribal Technical Advisory Group (TTAG) Face to Face Meeting
What they are saying:
- Walter Murillo spoke about the importance of including UIOs in state Traditional Healing waivers allowing state Medicaid agencies to cover Traditional Healing services at IHS/Tribal/UIO facilities, and the need for 100% Federal Medical Assistance Percentage (FMAP) for services provided to Medicaid beneficiaries at UIOs.
- Drew Snyder, Director of the Center for Medicaid and CHIP Services, Deputy Administrator, committed to fruitful relationship with the TTAG on all matters that impact Tribal communities.
- Kitty Marx, Director of CMS Division of Tribal Affairs (DTA), is retiring. Dr. Susan Karol, Chief Medical Officer at DTA, will be Acting Director of DTA for 120 days, then they will be posting for a permanent position.
Tribal Coalition Update
NCUIH has joined forces with over 20 Tribal organizations to ensure current administrative actions do not harm Native people and the programs that serve them.
Recent Coalition Action:
- Sent letters on February 21 to HUD, Treasury, Defense, and Small Business Administration, and BIA secretaries regarding treatment of Tribal Nations in implementation of Administration priorities.
- Sent letters to Senate Leadership on February 20 and House Leadership on February 25 expressing concern and highlighting opportunities for Indian Country as Congress considers budget reconciliation legislation.
Learn more at www.thecoalitiongroup.net
Upcoming Events and Dates to Know
Upcoming Events
- April 7-10: Tribal Self-Governance Conference in Chandler, AZ. Register here.
- April 16: Next NCUIH Monthly Policy Workgroup (virtual).
- April 17: Office of Urban Indian Health Programs (OUIHIP) Urban Program Executive Directors/Chief Executive Officers Monthly Conference Call.
- April 22-23: HHS FY 2027 Annual Tribal Budget Consultation. Register here.
- April 22-25: NCUIH 2025 Annual Conference and Hill Day in Washington, D.C. Register here.
- April 24: 2nd 2025 HHS STAC Meeting.
- April 24: IHS Direct Service Tribe Advisory Committee (DSTAC) 3rd Quarterly Meeting.