On September 30, 2022, six members of the Senate Committee on Indian Affairs (SCIA) sent a letter to House leadership, Senate leadership, and the Appropriations Committee requesting advance appropriations for the Indian Health Service (IHS) in the final upcoming appropriations bill. This letter comes as a continued effort by the National Council of Urban Indian Health (NCUIH) and Indian Country to secure advance appropriations for IHS and ensure stable and predictable funding for healthcare services provided to American Indians/Alaska Natives (AI/ANs). Due to this robust advocacy, the Senate FY 2023 funding bill provides $5.577 billion of advance appropriations for IHS for FY 2024, however, the House bill failed to include advance appropriations.
Senators Brian Schatz (D-HI), Maria Cantwell (D-WA), John Tester (D-MT), Catherine Cortez Masto (D-NV), Tina Smith (D-MN), and Ben Ray Lujan (D-NM) urged Congressional leadership to include advance appropriations for IHS for FY 2024 in the final FY 2023 omnibus bill to protect IHS from temporary lapses in appropriations and continuing resolutions (CRs). The Senators emphasized that during the 2019 government shutdown, “IHS was the only federal health care entity forced to operate without appropriations, causing some Urban Indian Organizations to close their doors completely. This funding disruption resulted in some health providers being unable to provide patients with critical care and medication.” A CR was recently enacted on September 30 to avoid a government shutdown while Congress continues negotiations on the final FY 2023 appropriations bill, extending current funding levels for all normal government programs until December 16, 2022. Urban Indian organizations (UIOs) must continue to operate on less than the FY 2022 funding levels for FY 2023 despite rising costs of healthcare. On July 28, 2022, former Acting Director of IHS, Liz Fowler, stated in her testimony before the House Natural Resources Subcommittee for Indigenous Peoples, “While the IHS has received an exception apportionment to provide the full-year recurring base amounts to Tribal Health Programs operating their own programs through ISDEAA Title I contracts and Title V compacts since FY 2020, this option is not available during government shutdowns, and it is not available at all to IHS-operated health programs, or Urban Indian Organizations. As a result, Direct Service tribes, and American Indians and Alaska Natives served by Urban Indian Organizations are disproportionately affected by disruptions in federal appropriations.”
Full Text of Letter:
Dear Senate and House Leadership,
As members of the Senate Committee on Indian Affairs, we write to urge including advance appropriations for the Indian Health Service (IHS) for fiscal year 2024 (FY24) in the final fiscal year 2023 (FY23) appropriations bill. Providing advance appropriations will ensure that the federal government continues to uphold its trust and treaty obligations to 2.7 million American Indians and Alaska Natives who receive healthcare services at more than 600 IHS hospitals, clinics, and health stations throughout the nation.[1]
The Indian Health Care Improvement Act, along with the Snyder Act of 1921, provides the foundational basis for providing healthcare to American Indians and Alaska Natives through IHS, in partial fulfillment of the United States’ trust and treaty obligations. Yet, unlike the Veterans Health Administration (VHA) at the Department of Veteran’s Affairs, which receives the majority of its funding through advance appropriations, IHS is funded through annual appropriations.[2] We were therefore pleased to see $5.577 billion in advance appropriations included in the Senate-released draft Interior and Environment subcommittee appropriations bill.
Advance appropriations, particularly during temporary lapses in appropriations and continuing resolutions, would provide continued budget certainty and enable long term planning to maintain orderly and continuous operations of critical health programs for Native American communities. Budgetary uncertainty risks interruption of health services and reduction in quality of care. During the partial government shutdown in 2019, for example, IHS was the only federal health care entity forced to operate without appropriations, causing some Urban Indian Organizations to close their doors completely. This funding disruption resulted in some health providers being unable to provide patients with critical care and medication.[3] Additional, and preventable, funding uncertainty impacts include risk of downgraded credit ratings on commercial loans secured by Tribes and Urban Indian Organizations; challenges related to recruitment and retention of healthcare providers; increased administrative burden and costs, such as employee furloughs and terminations; and other negative financial effects on Tribes.[4]
It is critical that advance appropriations are included in the FY23 omnibus appropriations bill. Given the impacts of uncertain funding, the lack of parity with VHA, and the unique trust relationship between the United States and American Indians and Alaska Natives, future year funding is necessary. We look forward to working with you to pass this critical legislation.
Thank you for your consideration of our request.
Background on Advance Appropriations for IHS
Advance appropriations are appropriations that become available one year or more after the year for which the appropriations act is passed. The Indian healthcare system, which includes IHS facilities, Tribal facilities, and UIOs, is the only major federal healthcare provider funded through annual appropriations. Funding through annual appropriations leads to funding uncertainty because the availability and amount of the appropriation is subject to the annual budget negotiation process. If IHS were to receive advance appropriations, it would not be subject to government shutdowns, automatic sequestration cuts, and CRs as its funding for the next year would already be in place. Congress recently enacted a CR, which passed the House by a vote of 230-201 and Senate by a vote of 75-25, to keep the government funded until December 16. UIOs must continue to operate on FY 2022 funding levels for FY2023 despite rising costs of healthcare.
Lapses in federal funding risk AI/AN lives. Every year, on average, Congress passes five continuing resolutions to keep the government open while Congress reaches a budget agreement, and there were long government shutdowns in 1996, 2013, and 2019. During the FY 2019 shutdown, several UIOs did not have adequate funding to maintain normal operations and were required to reduce services, lose staff, or close their doors entirely, putting the health and well-being of their patients at risk. In a UIO shutdown survey, five out of thirteen UIOs indicated that they could only maintain normal operations for 30 days without federal funding. One UIO suffered seven opioid overdoses, five of which were fatal.
Resources on Advance Appropriations for IHS:
NCUIH and Indian Country Advocacy
NCUIH, along with three other national Native organizations, the National Indian Health Board (NIHB), National Congress of American Indians (NCAI), United South and Easter Tribes (USET), have been advocating on behalf of advance appropriations for almost a decade and have passed resolutions supporting advance appropriations for IHS.
On January 17, 2019, NCUIH sent a letter to the Vice Chairman of the Senate Committee on Indian Affairs (SCIA), Tom Udall, in support of IHS advance appropriations legislation. On March 9, 2022, NCUIH joined NIHB and over seventy Tribal nations and national Indian organizations in sending a series of joint letters to Congress requesting advance appropriations for IHS in the FY 2022 omnibus. On June 16, 2022, NIHB and NCAI published a legislative action alert requesting that SCIA support and include IHS advance appropriations in the current FY 2023 appropriations bill. Most recently, NCUIH sent letters to Speaker Pelosi, House Minority Leader McCarthy, Senate Majority Leader Schumer, Senate Minority Leader McConnell, Senate Interior Appropriations Committee, and SCIA to support advance appropriations for IHS.
Federal and Congressional Support
There has also been strong long-standing support from Congress on this issue. Before the recent SCIA letter to Congressional leadership urging advance appropriations for IHS in the final FY 2023 appropriations bill, the Native American Caucus also sent a letter to House Appropriations Committee Chair DeLauro and Ranking Member Granger requesting that advance appropriations for IHS for FY 2023 be included in the final FY 2022 appropriations bill on January 12, 2022. On June 3, the Native American Caucus sent another letter encouraging the Committee to work towards shifting IHS from discretionary to mandatory funding and requesting that, while this shift is underway, the Committee include advanced appropriations for IHS in the final FY 2023 Appropriations bill.
On April 25, 2022, a bipartisan group of 28 Representatives requested up to $949.9 million for urban Indian health in FY 2023 and advance appropriations for IHS until such time that authorizers move IHS to mandatory spending, and 12 Senators sent a letter with the same requests. Last year, for the first time ever, the Senate Appropriations Committee included an additional $6.58 billion in advance appropriations to IHS for FY 2023 in its FY 2022 Interior, Environment, and Related Agencies bill.
Back in 2014, SCIA held its first hearing on advance appropriation bill Indian Health Service Advance Appropriations Act of 2013 (S. 1570). In a 2019 House Natural Resources Subcommittee for Indigenous Peoples (SCIP) hearing on advance appropriations bills H.R. 1128 and H.R. 1135, former IHS Principal Deputy Director, Rear Admiral Michael Weahkee, reaffirmed Indian Country’s repeated request for advance appropriations stating that “[t]hrough the IHS’s robust annual Tribal Budget Consultation process, Tribal and Urban Indian Organization leaders have repeatedly and strongly recommended advance appropriations for the IHS as an essential means for ensuring continued access to critical health care services. The Department continues to hear directly from tribes advocating support for legislative language that would provide the authority of advance appropriations for the IHS. The issues that Tribes have identified present real challenges in Indian Country and we are eager to work with Congress on a variety of solutions.” More recently on July 28, 2022, IHS Acting Deputy Director Elizabeth Fowler reaffirmed IHS’s support for advance appropriations during a SCIP hearing on the Indian Health Service Advance Appropriations Act (H.R. 5549) stating that “[IHS] remain[s] firmly committed to improving quality, safety, and access to health care for American Indians and Alaskan Natives. Mandatory funding and advanced appropriations are necessary and critical steps toward that goal… [I] urge the House to act on advanced appropriations through the appropriations process with or without the authorizing legislation that is the subject of this hearing.”
The U.S. Commission on Civil Rights report from 2018, “Broken Promises: Continuing Federal Funding Shortfall for Native Americans” serves as another benchmark of support by including advance appropriations for IHS as a key recommendation to the federal government to ensure greater funding stability for IHS.
History of Advance Appropriations Bills
Legislation on this effort has been introduced in 11 bills since 2013:
- 10/2013 – Indian Health Service Advance Appropriations Act of 2013 (3229/S. 1570)
- Sponsor: Rep. Don Young/Sen. Lisa Murkowski
- 1/2015 – Indian Health Service Advance Appropriations Act of 2015 (395)
- Sponsor: Rep. Don Young
- 1/2017 – Indian Health Service Advance Appropriations Act of 2017 (235)
- Sponsor: Rep. Don Young
- 2/2019 – Indian Programs Advance Appropriations Act (1128/S. 229)
- Sponsor: Rep. Betty McCollum/Sen. Tom Udall
- 2/2019 – Indian Health Service Advance Appropriations Act of 2019 (1135/S. 2541)
- Sponsor: Rep. Don Young/Sen. Lisa Murkowski
- 10/2021 – Indian Health Service Advance Appropriations Act (5549)
- Sponsor: Rep. Don Young
- 10/2021 – Indian Programs Advance Appropriations Act of 2021 (5567/S. 2985)
- Sponsor: Rep. Betty McCollum/Sen. Ben Ray Lujan
Next Steps
Congress will have until December 16, 2022 to pass a longer-term spending package for FY 2023. In the meantime, NCUIH will continue to advocate for advance appropriations in the final FY 2023 omnibus.
[1] Hybrid SCIP Legis. Hearing – July 28, 2022 Before the Subcomm. on Indigenous Peoples, 117th Cong. 2 (2022) (statement of Elizabeth Fowler, Acting Dir., Indian Health Serv.).
[2] ELAYNE HEISLER & KATE MCCLANAHAN, CONG. RESEARCH SERV., R46265, ADVANCE APPROPRIATIONS FOR THE INDIAN HEALTH SERVICE: ISSUES AND OPTIONS FOR CONGRESS (2020).
[3] Hybrid SCIP Legis. Hearing – July 28, 2022 Before the Subcomm. on Indigenous Peoples, 117th Cong. 2 (2022) (statement of Maureen Rosette, Chief Operating Officer, NATIVE Project).
[4] GAO-18-652 (Sept. 2018), INDIAN HEALTH SERVICE: CONSIDERATIONS RELATED TO PROVIDING ADVANCE APPROPRIATIONS AUTHORITY, available at https://www.gao.gov/assets/700/694625.pdf.



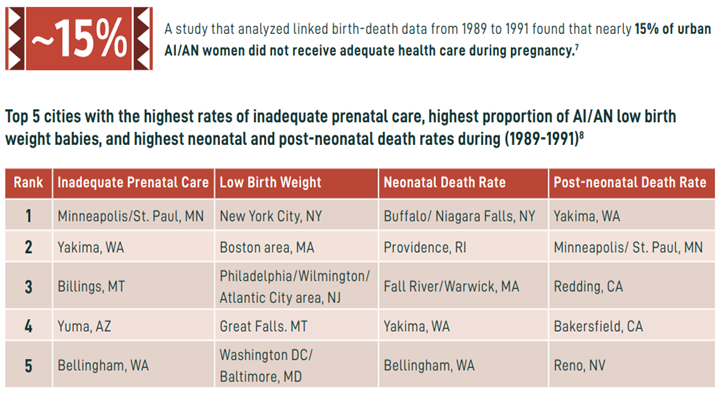
 Raimondi highlighted that “over half of urban Indian health centers provide care for maternal health, infant health, prenatal, and/or family planning. However, due to chronic underfunding, many of these health centers only have the capacity to carry out these services for the early stages of pregnancy.” She continued to say, “despite desiring to do so, many urban Indian health clinics cannot expand their services to provide complete care for mothers and infants from conception to birth due to underfunding.” Raimondi provided the following recommendations to the Advisory Committee:
Raimondi highlighted that “over half of urban Indian health centers provide care for maternal health, infant health, prenatal, and/or family planning. However, due to chronic underfunding, many of these health centers only have the capacity to carry out these services for the early stages of pregnancy.” She continued to say, “despite desiring to do so, many urban Indian health clinics cannot expand their services to provide complete care for mothers and infants from conception to birth due to underfunding.” Raimondi provided the following recommendations to the Advisory Committee:




 On September 27, 2022, NCUIH attended the swearing-in of the new Indian Health Service (IHS) Director Roselyn Tso (Navajo). NCUIH’s CEO Francys Crevier (Algonquin) and Board President-Elect and CEO of Native Health in Phoenix, Arizona Walter Murillo (Choctaw) were in attendance. Prior to Director Tso’s swearing-in, IHS was without a permanent director for 21 months.
On September 27, 2022, NCUIH attended the swearing-in of the new Indian Health Service (IHS) Director Roselyn Tso (Navajo). NCUIH’s CEO Francys Crevier (Algonquin) and Board President-Elect and CEO of Native Health in Phoenix, Arizona Walter Murillo (Choctaw) were in attendance. Prior to Director Tso’s swearing-in, IHS was without a permanent director for 21 months.