November Policy Updates: Annual Policy Assessment, Vaccine Toolkit, Medicaid Advocacy on the Hill, and more!
RSV & flu Vaccine Toolkit, Policy Assessment, and Annual Report: Explore vaccination resources for Native communities and highlights from NCUIH’s latest Annual Report.
🔍 FY 2027 Area Budget Consultations: UIO Engagement Matters!
📜 Appropriations Update: Congress is back to address funding priorities, including the NDAA and expiring Continuing Resolution.
🗳 2024 Election Results Analysis: An overview of the House and Senate and key race outcomes.
💡 FMAP and SDPI Updates: Advocacy efforts continue for Medicaid parity, with renewed momentum for year-end SPDI reauthorization.
🎤Advocacy: NCUIH Joins CMS Tribal Technical Advisory Group in Key Medicaid Discussions before CMS Leadership and Senate Committees: Traditional Healing Waivers, Medicaid Fraud, and 100% FMAP for UIOs.
📅 Upcoming Federal Agency Comments: Key comment deadlines from SAMHSA, IHS, and SSA on policies affecting Native health.
📬 ICYMI: Updates on IHS Tribal Consultation policy and NIH’s policies on Tribal biospecimens.
🔎 NCUIH in Action: Recap of NCUIH’s role at the NCAI Annual Convention, White House Traditional Healing Summit, and American Cancer Society Cancer Action Network Panel discussions.
📆 Important Dates and Events: Upcoming events, from federal Tribal Advisory Committees to the White House
Hot off the Press: RSV and Flu Vaccine Toolkit, Annual Policy Assessment, and 2024 Annual Report

New Release: RSV and Flu Vaccine Toolkit
NCUIH has launched a comprehensive RSV and flu vaccine toolkit to support Urban Indian Organizations (UIOs) in promoting respiratory syncytial virus (RSV) and flu vaccinations within Native communities. The toolkit offers valuable resources, educational materials, and outreach strategies to help UIOs raise awareness and increase vaccination uptake in American Indian and Alaska Native (AI/AN) populations. The toolkit features social media graphics and customizable posts, posters to download and print, and messaging templates for use in newsletters or flyers. By using these materials, we hope you will reach more people in your community and encourage greater RSV and flu vaccine uptake during this critical time.
- Access the toolkit here.
2024 Annual Policy Assessment
NCUIH is pleased to announce the release of its 2024 Policy Assessment. In September, NCUIH hosted five focus groups to identify UIO policy priorities for 2025 as they relate to the IHS designated facility types (full ambulatory, limited ambulatory, outreach and referral, and outpatient and residential). Together, these focus groups allow NCUIH to work with UIOs to identify policy priorities in 2025 and barriers that impact the delivery of care to Native patients and their communities.
- Access the assessment here.
Annual Report Now Available!
NCUIH’s 2024 Annual Report is now live on our website, providing an in-depth look at our efforts and accomplishments over the past year. This report highlights:
- Key Achievements in advocacy, policy, and health initiatives supporting urban Native communities.
- Partnerships and Collaborations that have strengthened resources for Urban Indian health.
- Data and Insights showcasing trends, challenges, and successes in Urban Indian health initiatives, including outcomes of vaccination and public health campaigns.
- Future Goals and Strategic Initiatives to further advance health equity, access to care, and wellness for Native communities across the country.
The report is a valuable resource for understanding the impact of NCUIH’s work and our continued commitment to supporting UIOs and Native health. Visit our website to read the full report and explore how NCUIH is working to drive positive change in Native communities.
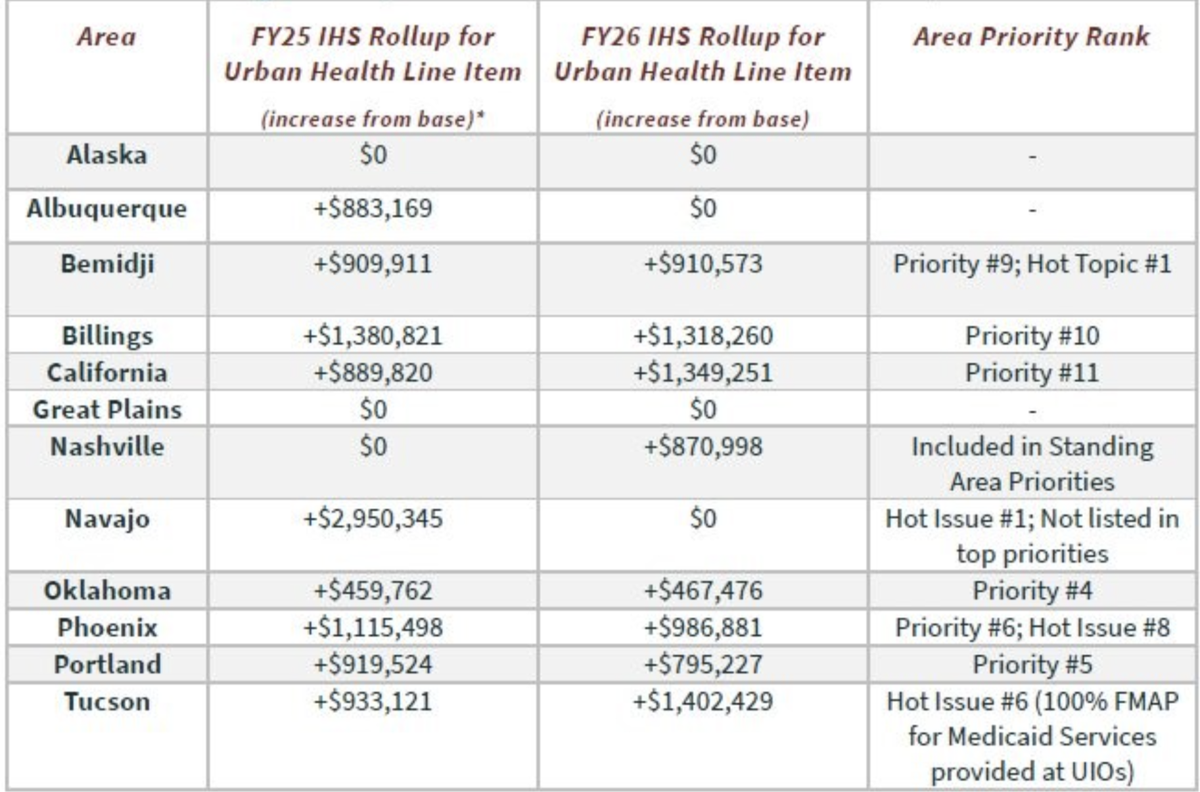
Area Budget Formulation – Your Engagement Matters!
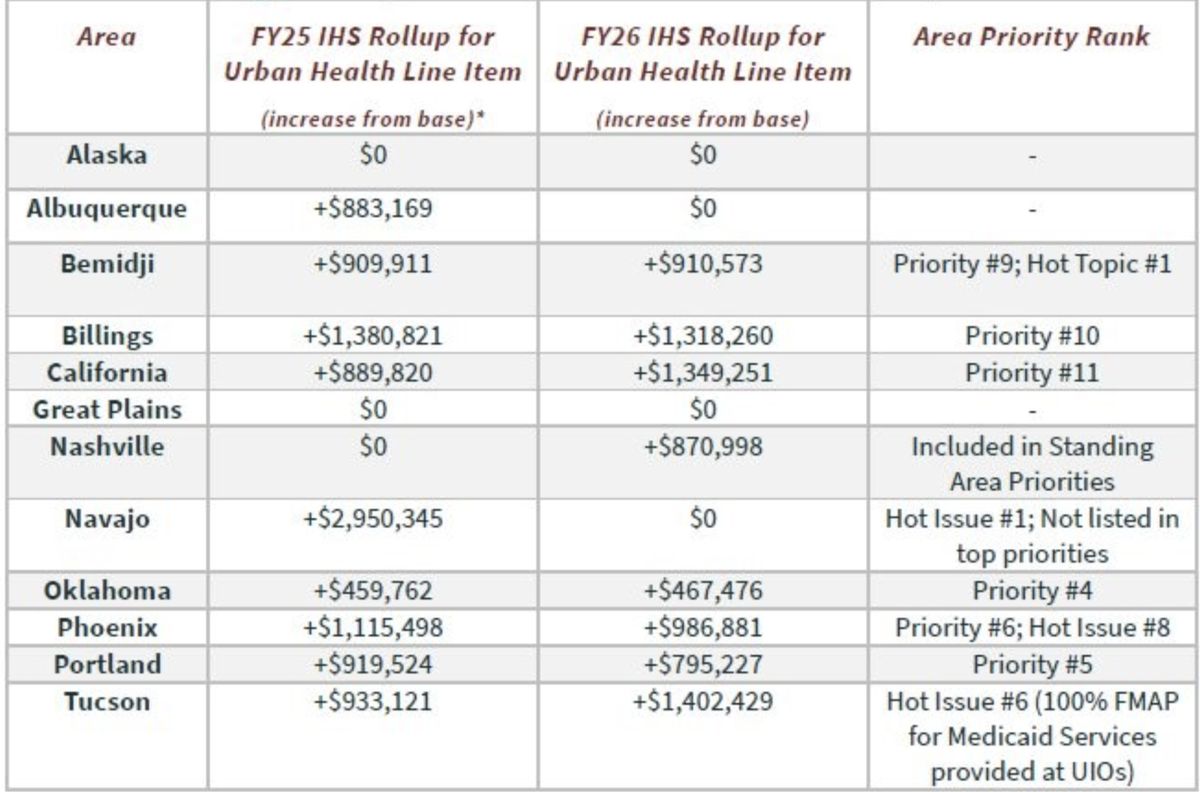
Why Should UIOs Attend?
- Each Area submits its recommendation to the National Workgroup.
- We believe that your attendance at Budget Formulation is directly linked to the recommendations and rankings for each area.
- The average of all these amounts is used to calculate the Urban Line item.
- If you are unable to attend your Area Budget Consultation when it is announced, please contact NCUIH. You may be able to submit testimony and/or slides to ensure your UIO’s contribution to the Area.
Upcoming Area Budget Consultation Meeting Dates:
- Great Plains: 12/12/2024 (in-person). More information here.
- Portland: TBD
Technical Assistance: If your UIO would like to schedule a one-on-one session with NCUIH to prepare for your respective Area budget consultation, please don’t hesitate to reach out to policy@ncuih.org.
Appropriations Update: Fiscal Year 2025

Congress Returns for Lame Duck Session
On November 12, Congress resumed its legislative session, entering a period where lawmakers face several high-stakes decisions before the year’s end.
Top Priorities for the Lame Duck Session:
- Government Funding
- National Defense Authorization Act (NDAA)
- Public Health Extenders
Current Situation:
The current Continuing Resolution (CR) is set to expire on December 20, 2024. Congress must decide on a path forward to avoid a government shutdown.
What’s at Stake:
Congressional discussions are underway on two main options:
- Full-Year Spending Package: A comprehensive budget for Fiscal Year 2025, providing funding stability for the next year.
- Short-Term Continuing Resolution: Extends funding through the start of the new Congress and Administration, delaying a full-year budget decision.
Key Players & Positions:
- House Majority Leaders favor a short-term extender, aiming to pass minimal budget extensions until the next Congress.
- Senate Democrats are expected to push for a more comprehensive spending package.
What’s Next:
Congressional leaders continue to negotiate a plan before the December deadline.
2024 Election Results Analysis
Senate:
Republicans have secured control of the Senate with 53 seats, while Democrats hold 47 seats. Senator John Thune (R-SD) has been elected as the new Senate Majority Leader.
House of Representatives:
Republicans have achieved a majority in the House, securing 219 seats, while Democrats hold 213 seats, with several races still pending.
Key Race Outcomes:
- Rep. Tom Cole (R-OK), Rep. Sharice Davids (D-KS), Rep. David Valadao (R-CA), and Rep. Don Bacon (R-NE) have all been re-elected.
FMAP and SDPI Updates: Fiscal Year 2025

Federal Medical Assistance Percentage (FMAP) Update:
NCUIH remains committed to advocating for the inclusion of the Urban Indian Health Parity Act in any year-end legislative packages.
How UIOs Can Help:
- Sign Letter of Support: NCUIH is leading a partnership sign on letter asking House and Senate Leadership to include 100% FMAP for UIOs in any end-of-year health extender. To support this advocacy letter, sign on to the letter through this form by COB Friday November 29, 2024. Please share the letter with any partner organizations who might want to support this issue. Please reach out to policy@ncuih.org with any questions.
- Seek Tribal Support: We are also seeking Tribal letters of support. If you know of any Tribes willing to provide a letter, please connect with us at policy@ncuih.org.
- Important Reminder: Even without 100% FMAP, UIOs can collaborate with their states to negotiate improved reimbursement rates.
Special Diabetes Program for Indians (SDPI) Update:
The SDPI was reauthorized in the March 2024 Consolidated Appropriations Act and is funded through December 31, 2024.
Current Advocacy Efforts:
- Congressional Letter: On November 12, 2024, 55 Senators sent a Dear Colleague Letter requesting Senate Leadership prioritize reauthorizing SDPI in an end-of-year funding package.
A Dear Colleague letter is also circulating through the U.S House of Representatives. - NCUIH’s Support: On November 19, 2024, NCUIH also sent a letter to Congressional leadership to advocate for SDPI’s continued funding and support.
NCUIH Joins CMS Tribal Technical Advisory Group in Key Medicaid Discussions before CMS Leadership and Senate Committees: Traditional Healing Waivers, Medicaid Fraud, and 100% FMAP for UIOs
Centers for Medicare & Medicaid Services (CMS) Tribal Technical Advisory Group (TTAG) Hybrid Face-to-Face Meeting

NCUIH President and TTAG Representative Walter Murillo (Choctaw) speaks before the CMS TTAG.
On November 6-7, NCUIH President and TTAG Representative Walter Murillo, represented NCUIH at the CMS TTAG meeting in Washington D.C., the meeting covered:
- Traditional Healing Waivers: The CMS’ State Demonstrations Group presented approvals for waivers related to Traditional Health Care practices, with CMS collaborating with states on monitoring and evaluation processes.
- Arizona Medicaid Fraud: Mr. Murillo spoke before CMS leadership to address the severe impact of Medicaid fraud involving human trafficking and fraudulent billing in Arizona, which has strained IHS, Tribal, and UIO resources. He urged CMS to take corrective action to protect Native beneficiaries.
Senate Hill Staff Briefing on CMS TTAG Legislative Priorities
NCUIH CEO Francys Crevier (Algonquin) speaks before the CMS TTAG Senate briefing.
On November 21, the CMS TTAG hosted a briefing for the Senate Committee on Indian Affairs (SCIA), the Senate Health, Education, Labor and Pensions (HELP) Committee, and the Senate Finance Committee majority and minority staff on TTAG legislative priorities—primarily Medicaid or Medicare issues.
NCUIH CEO Francys Crevier discussed the policy priority of 100% FMAP for UIOs and requested that, during this lame duck, this legislative fix be included in any end-of-year health extender package or omnibus.
Upcoming Federal Agency Comment Opportunities
November 27 – Substance Abuse and Mental Health Services Administration (SAMHSA) Tribal Behavioral Health (TBH) Grant Program
- Overview: SAMHSA is redesigning the Tribal Behavioral Health program Notice of Funding Opportunity (NOFO) to streamline the application process and allow Tribes to select from two prevention priorities:
– One NOFO focused on suicide prevention
– One NOFO focused on substance use prevention - SAMHSA held a Tribal Consultation on November 21.
- Comment Deadline: November 27, 2024. Email to otap@samhsa.hhs.gov.
December 6 – U.S. Department of Health and Human Services (HHS) Request for Information (RFI) on 2026-2030 National HIV/AIDS and Related Strategic Plans
- Request for Input: The Office of Infectious Disease and HIV/AIDS Policy is gathering feedback on upcoming strategic plans:
– National HIV/AIDS Strategy for the United States: 2026-2030
– Sexually Transmitted Infections National Strategic Plan for the United States: 2026-2030
– Vaccines National Strategic Plan for the United States: 2026-2030
– Viral Hepatitis National Strategic Plan for the United States: 2026-2030 - Comment Deadline: December 6, 2024. Submit electronically here.
December 6 – IHS Health Information Technology (HIT) Modernization Site Readiness and Training
- Tribal Consultation and Urban Confer Recap: The final IHS Tribal Consultation and Urban Confer session on HIT Modernization was held on November 7 regarding Site Readiness and Training.
Key Questions for Feedback:
– What elements of the site readiness and training approach should the IHS consider to support UIOs pre- and post-go-live?
– What challenges might your organization face in assessing readiness for deployment?
– What are the site-level needs that the IHS should consider when designing and deploying Public Health Analytics and Technology (PATH) Electronic Health Records (EHR) training?
- Comment Deadline: December 6, 2024. Email consultation comments to consultation@ihs.gov and confer comments to urbanconfer@ihs.gov with the subject line: Health IT Modernization.
December 13 – Social Security Administration (SSA) Tribal Consultation on Call to Action Plan
- Tribal Consultation Recap: SSA’s Tribal Consultation on November 14 sought input on the SSA Tribal Consultation Call to Action Plan and is seeking additional comments the Action Plan that seeks to expand partnerships across federal agencies to UIOs.
- Key Initiative: The action plan emphasizes “Providing Tribal Consultation with Tribal Leaders and Urban Indian Organizations.”
- Comment Deadline: December 13, 2024. Email to aian.ec@ssa.gov.
December 16 – IHS Headquarters Office of Director Structure Reorganization
- Tribal Consultation and Urban Confer Recap: IHS held an Urban Confer on November 13 and Tribal Consultation on November 14 seeking comments and recommendations on the proposed reorganization of the IHS Headquarters Office under the Deputy Director for Intergovernmental Affairs (DDIGA). NCUIH hosted a prep session for UIOs on November 12.
- One IHS Initiative: Aims to improve coordination and efficiency across the agency.
- This reorganization may have significant impacts on how UIOs engage with IHS and the broader system.
- Comment Deadline: December 16, 2024 (tentative). Email consultation comments to consultation@ihs.gov and confer comments to urbanconfer@ihs.gov with the subject line: Proposed Reorganization of DDIGA Offices.
ICYMI: Recent Dear Tribal and Urban Leader Letters
Recent Dear Tribal and Urban Leader Letters (DTLL/DULL)
October 30 DTLL/DULL– National Institutes of Health (NIH) Tribal Consultation on “Disposition of Biospecimens Collected from Tribal Populations”
- Overview: NIH has proposed options for managing deidentified biospecimens collected from Tribal and international Indigenous populations, including returning them to Tribal authorities.
- Objective: The consultation aims to finalize options that honor Tribal sovereignty and cultural considerations, particularly when a Tribe has requested the return or transfer of biospecimens.
- Virtual Tribal Consultation: Thursday, December 5, 2024, from 11:00 AM to 1:00 PM ET. Register here.
- Written Testimony Deadline: January 20, 2025. Email to NIHTribalConsultation@nih.gov.
November 12 DTLL – IHS Publishes Updated IHS Tribal Consultation Policy
- Overview: This updated policy aims to reaffirm the IHS’ commitment to engage in regular, meaningful, and robust Tribal consultation.
- The updated policy reiterates that statutes and policies exist that require the IHS to confer with UIOs on the IHS budget formulation.
NCUIH in Action

NCUIH President Walter Murillo (Choctaw) addressing the General Assembly at the NCAI Annual Convention & Marketplace.
NCUIH at the National Congress of American Indians (NCAI) Annual Convention & Marketplace
On October 28-November 1, NCUIH represented UIOs at the 2024 National Congress of American Indians (NCAI) Annual Convention & Marketplace. During the convention, NCUIH presented key policy updates and introduced our Behavioral Health Financing Toolkit to the Health Subcommittee, co-chaired by NCUIH President Walter Murillo.
In addition to policy presentations, Mr. Murillo addressed the convention’s General Assembly, underscoring NCUIH’s commitment to advancing Urban Indian health and engaging Tribal leaders on critical health issues impacting all Native communities.
2nd Annual Traditional Healing Summit

NCUIH Board Member and Native American Health Center CEO Natalie Aguilera (Choctaw) with IHS Director Roselyn Tso (Navajo) at the White House Traditional Healing Summit.
On November 18-19, NCUIH Board Member and Native American Health Center CEO Natalie Aguilera, and NCUIH staff participated in the 2nd Annual Traditional Healing Summit hosted by HHS, in coordination with the White House Council on Native American Affairs.
House Democratic Caucus Native American Heritage Month Reception
On November 18, NCUIH staff joined the House Democratic Caucus Chair Pete Aguilar, Rep. Sharice Davids, Rep. Teresa Leger Fernández, Rep. Raúl Grijalva, Rep. Betty McCollum, Rep. Mary Peltola, Rep. Raul Ruiz, and Rep. Jill Tokuda for a reception in celebration of Native American Heritage Month.
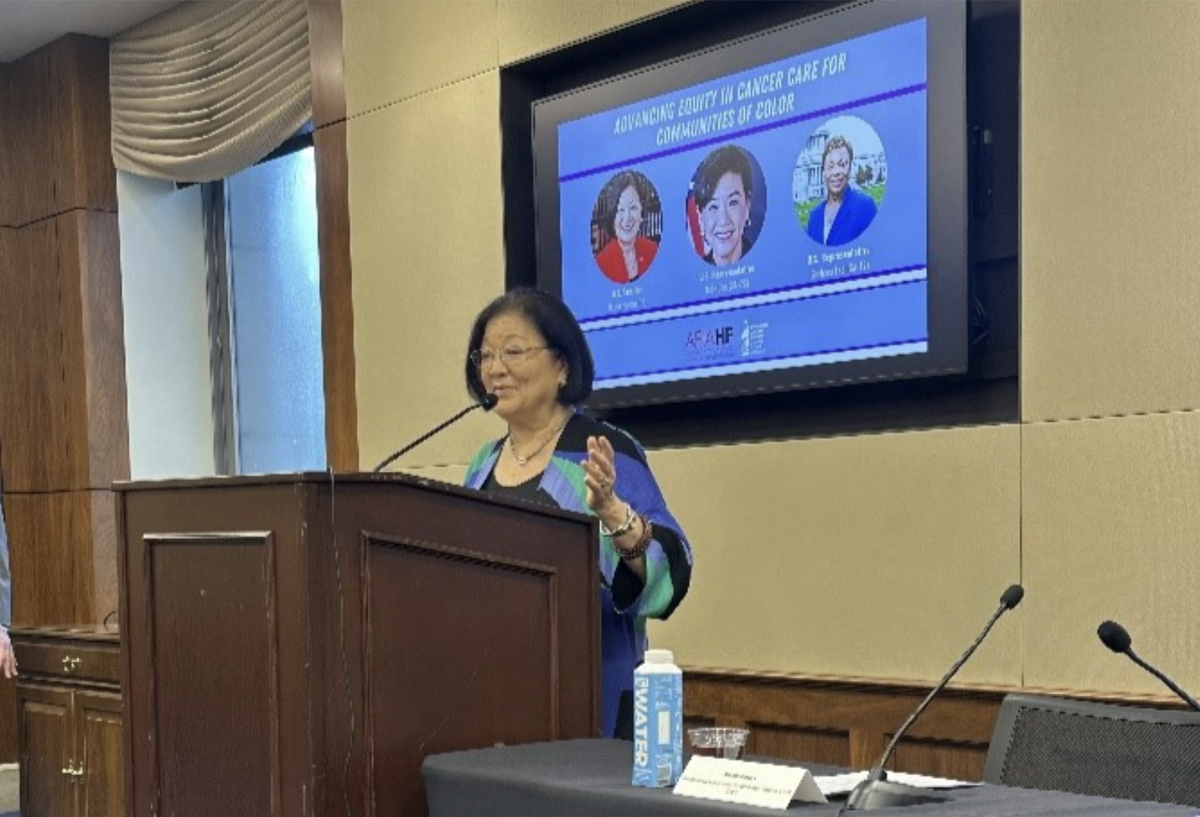
NCUIH Panel at the American Cancer Society Cancer Action Network Priorities and Partners Meeting

NCUIH CEO Francys Crevier (Algonquin) speaks at the ACS CAN Priorities and Partners Meeting Panel.
On November 20, NCUIH CEO Francys Crevier represented UIOs at an American Cancer Society Cancer Action Network (ACS CAN) Priorities and Partners Meeting Panel: High Risk Cancer and Policy Solutions alongside Panel Moderator Faith Nyong, PhD, Ascension Mercy, and panelists: Cyndie Navarro-Davila, Director of State and Local Campaigns – Health Equity at ACS CAN; Rod Lew, Executive Director of Asian Pacific Partners for Empowerment Advocacy and Leadership (APPEAL); Lauren Davis, Patient Advocacy Relations at Genentech; and Dr. Scout, Executive Director of National LGBTQI Cancer Network.
Ms. Crevier emphasized UIOs’ critical role in lifesaving care and highlighted the need for mandatory IHS funding and 100% FMAP for UIOs to ensure equitable health care for urban Native patients.
Upcoming Events and Important Dates
December 9 – White House Tribal Nations Summit
December 15-18 – IHS Tribal Self-Governance Advisory Committee (TSGAC) Meeting in Washington, D.C.
December 19 – Office of Urban Indian Health Programs (OUIHIP) Monthly Conference Call for UIO Executive Directors and CEOs