Indian Health Budget Updates
- Yesterday, President Biden released the annual budget proposal for Fiscal Year (FY) 2024. The Budget proposes $9.7 billion for the Indian Health Service (IHS), an increase of $2.5 billion or 36% above FY23 enacted levels.
- NCUIH CEO Francys Crevier testified before Congress, and Committee leaders pledged to protect the Indian Health Service budget from cuts.
Read on to learn more.
Biden Budget Proposal Demonstrates Continued Commitment to Improving the Indian Health Service
On March 9, 2023, the President released the annual budget proposal for Fiscal Year (FY) 2024. The “HHS Budget in Brief” has been released but the Congressional Justification for the Indian Health Service has not been released.
The bottom line: Mandatory Funding for IHS Remains a Priority; Advance Funding Still Needed
What they’re saying: “The Administration is committed to upholding the United States’ trust responsibility to tribal nations by addressing the historical underfunding of IHS. The enactment of an advance appropriation for 2024 for IHS was a historic and welcome step toward the goal of securing adequate and stable funding to improve the overall health status of American Indians and Alaska Natives.”
- The budget proposal includes the Administration’s commitment that by 2025, the IHS budget would shift from mostly discretionary to all mandatory funding.
- The President also reaffirmed that “until [mandatory funding] is enacted, it is critical that Congress continue to prioritize advance appropriations for IHS through the discretionary appropriations process to ensure funding for healthcare services and critical facilities activities are not disrupted.”
In Context: This proposal falls short of the Tribal Budget Formulation Workgroup (TBFWG)’s request of $51.4 billion for IHS for FY24.
The big picture: NCUIH will continue to advocate for the Tribal Budget Formulation Workgroup requests for urban Indian health and the Indian Health Service.
What’s next: Congress will hold hearings to review the President’s request. House Republicans are calling for reduced spending levels, while Senate appropriators are having bipartisan talks on top-line totals, with a goal of starting spending bill markups as soon as May.
By the numbers:

This chart shows how the enacted amounts compare to the Tribal request and President proposals.
Overall Budget for Department of Health and Human Services (HHS)
- The Budget requests $144 billion in discretionary budget authority for FY24, a $14.8 billion or 11.5% increase from the FY23 enacted level.
Indian Health Service Budget Highlights
- Indian Health Service Overall: $9.7 billion, an increase of $2.5 billion or 36% above FY23 enacted and $41.7 billion less than requested by TBFWG.
- Urban Indian Health: $115 Million for an increase of $25 million or 27% above FY23 enacted and $858.6 million less than requested by the TBFWG.
- Reauthorizes and Increases Funding for the Special Diabetes Program for Indians: The budget proposes to reauthorize the Special Diabetes Program for Indians and provide $250 million in FY24, $260 million in FY25, and $270 million in FY26 in new mandatory funding.
- Proposes New Program to Increase Public Health Capacity and Infrastructure: The budget also proposes new funding of $150 million in FY25 to address public health capacity and infrastructure needs in Indian Country. This funding would support an innovative hub-and-spoke model to address local public health needs in partnership with tribes and urban Indian organizations.
Go deeper:
Bipartisan Pledge from House Committee Leaders to Protect Indian Health Service Budget from Budget Cuts

NCUIH CEO, Francys Crevier (Algonquin), testifies at American Indian and Alaska Native Public Witness Day.
On March 9, 2023, the National Council of Urban Indian Health CEO Francys Crevier (Algonquin), testified before the House Interior Appropriations Subcommittee as part of American Indian and Alaska Native (AI/AN) Public Witness Days regarding FY24 funding for the Indian Health Service. NCUIH was invited to testify on the critical health needs of American Indians and Alaska Natives living in urban areas.
Did you know?: It was the first hearing of this Subcommittee with the return of Chairman Mike Simpson.
NCUIH’s testimony called attention to the staggering health disparities that Native communities face and requested full funding for the Indian Health Service.
“Native people deserve full, healthy lives. We cannot continue to rely on short-term solutions that only address the symptoms of the problem. We ask for full funding for IHS and the urban Indian health line item. Make advance appropriations and 100% FMAP for UIOs permanent. Protect us from sequestration now.”
– Francys Crevier (Algonquin), NCUIH CEO
Following Ms. Crevier’s testimony, Chairman Simpson pledged to prioritize protecting the Indian health budget from the expected budget cuts.
“We are going to have to make sure that we prioritize Indian healthcare in these budgets…There are some areas we’re going to have to protect and Indian health is going to have to be one of them.”
-Chairman Mike Simpson (R-ID)
Ranking Member Chellie Pingree also attended and reaffirmed her continued commitment to prioritizing Native health care.
“Protecting Indian health is critically important, as is housing and education and so many other things, but meeting our treaty and trust obligations is just so critical… The idea that the budget is six, seven billion but should be 51, we just have to take a big leap at getting closer because you and the centers you represent know how to distribute and spend that money and know how to make sure we get access to it and that you can use it in the ways that its most important for [Tribes and Urban Indian Organizations].”
– Ranking Member Chellie Pingree (D-ME)
Our thought bubble: NCUIH applauds the bipartisan leadership of Chair and Ranking Member of the Appropriations Committee.
Go deeper:
- Read NCUIH’s written testimony.
- Watch NCUIH’s testimony.
What’s coming up next week?
- March 14 – 15, 2023 – Tribal Leaders Diabetes Quarterly Committee Meeting – Washington, DC (Event Website)
Thank you for your continued support and commitment to improving the lives of Native people.
 The National Council of Urban Indian Health (NCUIH) is pleased to announce the release of its
The National Council of Urban Indian Health (NCUIH) is pleased to announce the release of its 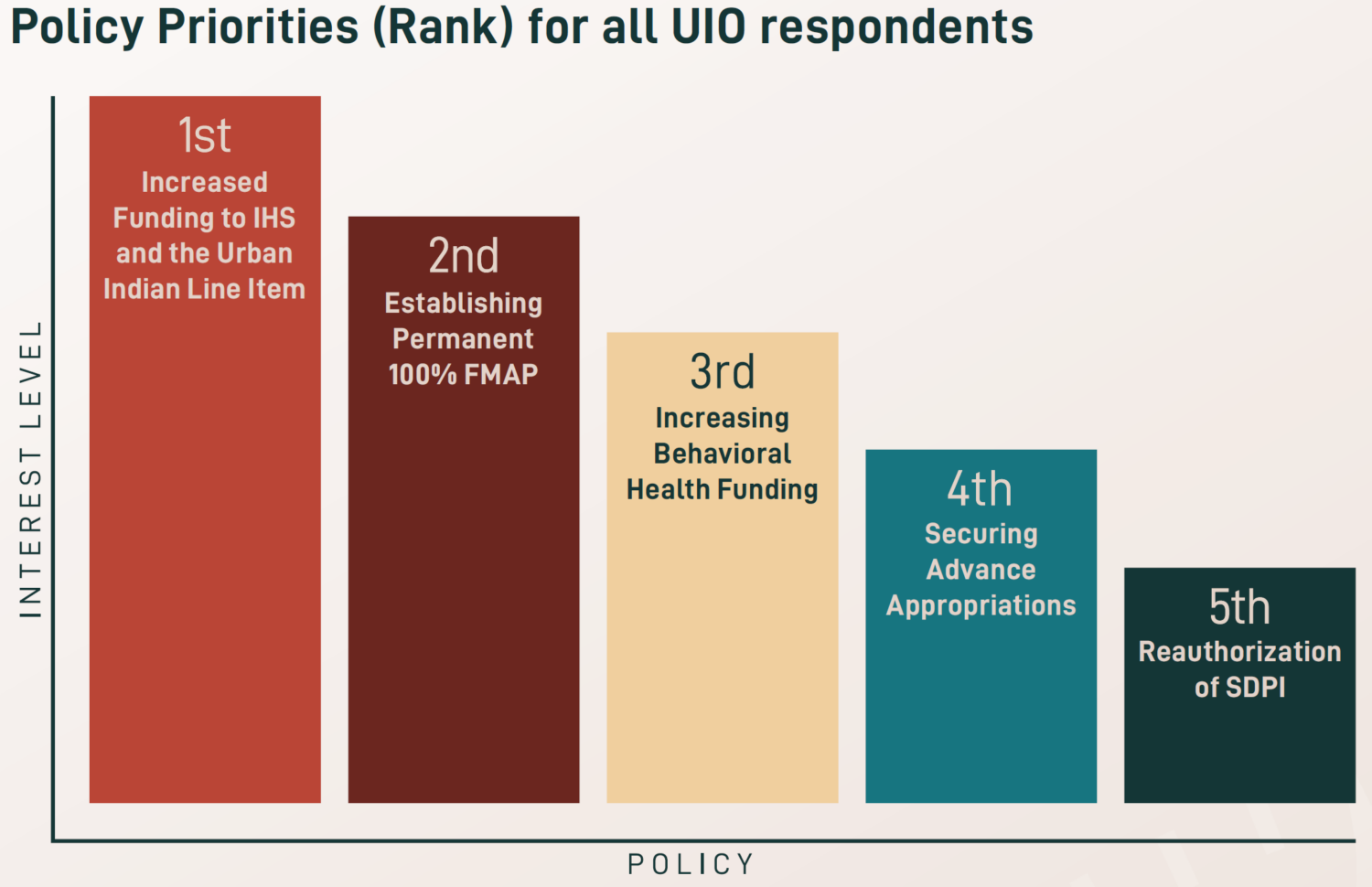 After the height of the COVID-19 pandemic, newfound priorities were identified for 2023, including workforce development and retention, increased funding for traditional healing, and expanded access to care and telehealth services. Existing priorities also remain a key focus across UIOs, especially increasing funding amounts for the urban Indian health line item and IHS, maintaining advance appropriations for IHS, establishing permanent 100% Federal Medical Assistance Percentage (FMAP) for UIOs, reauthorizing the Special Diabetes Program for Indians (SDPI), and increasing behavioral health funding.
After the height of the COVID-19 pandemic, newfound priorities were identified for 2023, including workforce development and retention, increased funding for traditional healing, and expanded access to care and telehealth services. Existing priorities also remain a key focus across UIOs, especially increasing funding amounts for the urban Indian health line item and IHS, maintaining advance appropriations for IHS, establishing permanent 100% Federal Medical Assistance Percentage (FMAP) for UIOs, reauthorizing the Special Diabetes Program for Indians (SDPI), and increasing behavioral health funding.