House Releases FY 2023 Appropriations Bill with $200 Million for Urban Indian Health, Fails to Include Advance Appropriations
The bill is to be considered by Full Committee this week and includes $8.1 billion for IHS, $1 billion less than the amount requested by the President.
Today, June 28, 2022, the House Appropriations Subcommittee on Interior, Environment, and Related Agencies released the Committee Bill Report for the fiscal year (FY) 2023 budget with $200 million for urban Indian health. The report and bill will be considered by the full House Appropriations Committee tomorrow morning and was approved by the House Subcommittee on Interior on June 21, 2022. The bill authorizes $8.1 billion for the Indian Health Service (IHS)— an increase of $1.5 billion from FY22 but $1 billion below the President’s request. Despite robust advocacy from Tribes and Urban Indian Organizations (UIOs), the bill does not include advance appropriations. Other key provisions include $17 million for generators for IHS/Tribal Health Programs/UIOs and $3 million for a Produce Prescription Pilot Program for Tribes and UIOs to increase access to produce and other traditional foods. A more detailed analysis follows below.
“NCUIH is grateful for the Committee’s inclusion of $200 million for urban Indian health for Fiscal Year 2023, but disappointed to see the reduced request from last year given all of the effects of COVID-19 and the growing costs of inflation. Unfortunately, the proposed amount would not fully fund the Indian Health Service and does not include critical advance appropriations. We especially thank Congresswoman McCollum and Ranking Member Joyce for their continued efforts to provide resources for Native healthcare and achieve advance appropriations. Too many Native lives have been lost during times of funding instability and we have had enough. We hope that House leaders will hear the calls of Indian Country to prioritize equity and provide stable funding for our health in accordance with the trust responsibility.” – Francys Crevier (Algonquin), CEO, NCUIH.
The President’s budget proposed to shift IHS from discretionary funding to mandatory funding in FY 2023. In the meantime, Native health advocates requested Advance Appropriations. To much disappointment, the House bill does not provide (or even mention) advance appropriations for IHS. Advance appropriations is a long-standing priority for Indian Country and advocates have been requesting Congress to provide stable funding for IHS especially considering the COVID-19 pandemic which has had tremendous, adverse impacts for American Indians and Alaska Natives. In the past month alone, NCUIH sent a letter to request Speaker Pelosi to allow for advance appropriations and NCAI and NIHB sent an action alert to request the Appropriations Committee include advance appropriations. Previously, NCUIH, along with 28 Representatives and 12 Senators requested advanced appropriations for IHS until such time that authorizers move IHS to mandatory spending.
- Bill Report with Urban Indian Health Line Item
- Draft House Interior Appropriations Bill
- Bill Summary
| Line Item | FY22 Enacted | FY23 TBFWG Request | FY23 President’s Budget |
FY23 House Proposed |
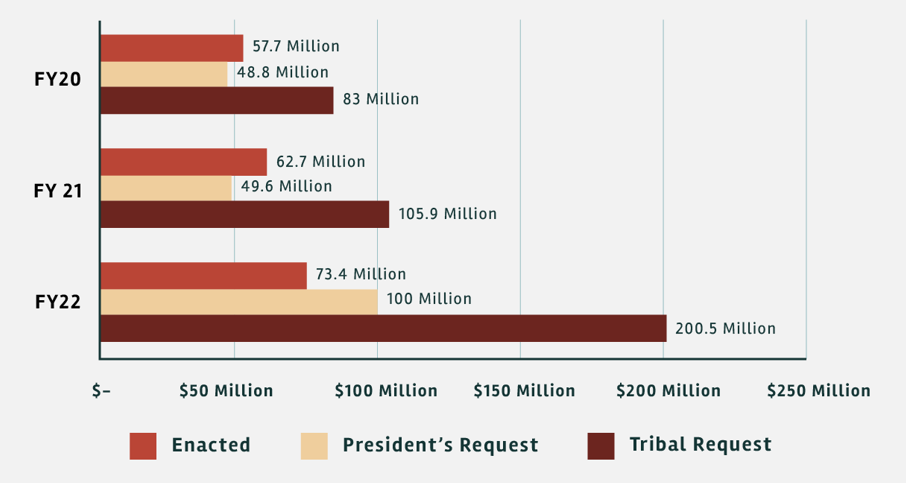
| Urban Indian Health | $73,424,000 | $949,900,000 | $112,514,000 | $200,000,000 |
| Indian Health Service | $6,630,986,000 | $49,800,000,000 | $9,100,000,000 | $8,100,000,000 |
Background and Advocacy
On March 28, 2022, President Biden released his budget request for Fiscal Year FY 2023 which included, for the first time ever, $9.3 billion in mandatory funding for IHS for the first year with increased funding each year over ten years. On April 25, 2022, the Indian Health Service (IHS) published their FY 2023 Congressional Justification with the full details of the President’s Budget, which included $112.5 million for Urban Indian Health— a 53.2% increase above the FY 2022 enacted amount of $73.4 million.
- IHS FY 2023 Congressional Justification
- President’s FY 2023 Budget
- NCUIH Analysis of President’s FY 2023 Budget
Full Funding, Advance Appropriations, and Mandatory Funding a Priority
NCUIH requested full funding for urban Indian health for FY 2023 at $949.9 million and at least $49.8 billion for IHS in accordance with the Tribal Budget Formulation Workgroup (TBFWG) recommendations. The marked increase for FY23 is a result of Tribal leaders, over several decades, providing budget recommendations to phase in funding increases over 10-12 years to address growing health disparities that have largely been ignored.
On April 5, 2022, NCUIH President-Elect and CEO of the Indian Health Center of Santa Clara Valley, Sonya Tetnowski (Makah Tribe), testified before and submitted public witness written testimony to the House Appropriations Subcommittee on Interior, Environment, and Related Agencies regarding FY 2023 funding for UIOs. NCUIH requested $49.8 billion for the Indian Health Service and $949.9 million for Urban Indian Health for FY 2023 as requested by the TBFWG, Advance appropriations for IHS, and support of mandatory funding for IHS including UIOs.
NCUIH recently worked closely with Representatives Gallego and Grijalva on leading a Congressional letter to the House Committee on Appropriations in support of increasing the urban Indian health line item for FY 2023. The letter has bipartisan support and calls for the highest possible funding for Urban Indian Health up to the TBFWG’s recommendation of $949.9 million and advanced appropriations for IHS until such time that authorizers move IHS to mandatory spending. On May 27, 2022, a group of 12 Senators sent a letter to the Senate Interior Appropriations Committee with the same requests.
During last week’s House Interior Subcommittee markup on the FY2023 funding bill, Rep. Chellie Pingree said of mandatory funding: “This shift requires legislative action by the authorizing committee, the House Committee on Natural Resources. In the absence of that legislation, I have included discretionary funding in this bill to ensure that there is no risk of a disruption in healthcare while that process is underway.”
Bill Highlights
Indian Health Service: $8.1 billion
- $8.1 billion for the Indian Health Service, an increase of $1.5 billion above the FY 2022 enacted level.
Urban Indian Health: $200 million
- Bill Report: “The recommendation includes $200,000,000 for Urban Indian Health, $126,576,000 above the enacted level and $200,000,000 above the budget request. This amount includes $31,000 transferred from the Alcohol and Substance Abuse Program as part of the for NIAAA program. The Committee expects the Service to continue including current services estimates for Urban Indian health in annual budget requests.”
Mandatory Funding:
- Bill Report: “For fiscal year 2023, the Administration proposed reclassifying IHS accounts as mandatory and did not submit a discretionary budget proposal. However, IHS did not provide implementation language and at the time of writing this report, the authorizing committees have not enacted the President’s proposal. Because the authorizing committees have not acted, the Committee is providing discretionary funds for IHS for fiscal year 2023 to ensure health care for Native Americans is not negatively impacted.”
- Note: There is no mention of advance appropriations for IHS in this bill.
Equipment: $118.5 million
- Bill Report: “The recommendation includes $118,511,000 for Equipment, $88,047,000 above the enacted level and $118,511,000 above the budget request. The bill continues $500,000 for TRANSAM.
- The report further states: “The Committee is aware that the increasing severity and frequency of extreme weather events has motivated certain jurisdictions to adopt de-energization protocols to reduce the risks of catastrophic wildfires. While these protocols are useful in limiting loss of life in affected communities, they can also have dire consequences for Tribal Health Programs located in impacted areas. To increase the resilience of these facilities, the recommendation includes an additional $17,000,000 to purchase generators for IHS, Tribal Health Programs, and Urban Indian Organizations located in areas impacted by de-energization events. In procuring backup generators, the Indian Health Service is directed to determine the most cost-effective method, which may include leasing. In determining the most cost-effective procurement method, the Service shall account for life-cycle maintenance costs associated with direct ownership and clinics’ capabilities to maintain these generators.”
Electronic Health Records: $284.5 million
- Bill Report: “To improve the current IT infrastructure system to support deployment of a new modern electronic health records (EHR) solution, the recommendation includes $284,500,000 for Electronic Health Records, $139,481,000 above the enacted level and $284,500,000 above the budget request.
- The report further states: “The Committee urges IHS to continue moving forward with modernizing its aging EHR system by replacing it with a solution that is interoperable with the new EHR at the Department of Veterans Affairs and with systems purchased by Tribes and UIOs. Modernization should include robust Tribal consultation and planning to ensure that Tribes and UIOs are enabled to take full advantage of resulting modern health information technology and are not unduly burdened during this process.”
Mental Health: $130 million
- Bill Report: “The recommendation includes $129,960,000 for Mental Health, $8,014,000 above the enacted level and $129,960,000 above the budget request.”
Alcohol and Substance Abuse: $264 million
- Bill Report: “The Committee provides $264,032,000 for Alcohol and Substance Abuse, $5,689,000 above the enacted level and $264,032,000 above the budget request. This amount transfers $31,000 to Urban Indians from the former National Institute on Alcohol Abuse and Alcoholism (NIAAA). Funding for Substance Abuse and Suicide Prevention grants is continued at fiscal year 2022 enacted levels.”
Community Health Aide Program (CHAP): $25 million
- Bill Report: “[…] an additional $20,000,000 is provided to expand the Community Health Aide Program to the lower 48 states with direction for IHS to report within 90 days of enactment of this Act on how funds will be distributed”
Tribal Epidemiology Centers: $34,433,361
- Bill Report: “[…] an additional $10,000,000 is for Tribal Epidemiology Centers”
Hepatitis C, HIV/AIDS and STDs Initiative: $52 million
- Bill Report: “[…] an additional $47,000,000 is for the Hepatitis C, HIV/AIDS and STDs initiative.”
Maternal Health: $10 million
- Bill Report: “The recommendation also includes an additional $4,000,000 to improve maternal health with continued direction to report to the Committee within 180 days of enactment of this Act on use of funds, updates on staff hiring, status of related standards, and the amount of training provided with these funds.”
Alzheimer’s Disease: $5.5 million
- Bill Report: “The recommendation maintains $5,500,000 to continue Alzheimer’s and related dementia activities at IHS. These funds will further efforts on Alzheimer’s awareness campaigns tailored for the AI/AN perspective to increase recognition of early signs of Alzheimer’s and other dementias; quarterly, competency-based training curriculum, either in-person or virtually, for primary care practitioners to ensure a core competency on assessing, diagnosing, and managing individuals with Alzheimer’s and other dementias; pilot programs to increase early detection and accurate diagnosis, including evidence based caregiver services within Indian Country, inclusive of urban Indian organizations (UIO); and an annual report to the Committee with data elements including the prevalence of Alzheimer’s incidence in the preceding year, and access to services within 90 days of the end of each fiscal year. The Committee continues direction to develop a plan, in consultation with Indian Tribes and urban confer with UIOs, to assist those with Alzheimer’s, the additional services required, and the costs associated with increasing Alzheimer’s patients and submit this information to Congress within 270 days of enactment of this Act.”
Produce Prescription Pilot Program:
- Bill Report: “The Committee continues $3,000,000 for IHS to create, in coordination with Tribes and UIOs, a pilot program to implement a produce prescription model to increase access to produce and other traditional foods among its service population. Within 60 days of enactment of this Act, the Committee expects IHS to explain how the funds are to be distributed and the metrics to be used to measure success of the pilot, which shall include engagement metrics, and may include appropriate health outcomes metrics, if feasible.”
Headache Disorders Centers of Excellence:
- Bill Report: “The Committee recognizes that over 560,000 people under IHS care are living with migraine or severe headache disorders and that AI/AN communities have the highest prevalence of both disabling headache disorders and concussion/mild traumatic brain injuries, among any racial or ethnic group in the United States. The Committee is concerned that AI/AN patients with chronic migraine, post-traumatic headache, and other disabling headache disorders often do not receive necessary specialty care. The IHS is encouraged to consider the feasibility of IHS Headache Centers of Excellence and if feasible, developing a budget proposal to establish IHS Headache Centers of Excellence to provide direct care, telehealth, and consultation patient services, as well as education and training.”