CMS Releases Medicaid Unwinding FAQs Document
On May 12, 2023, the Centers for Medicare and Medicaid Services (CMS) released a frequently asked questions (FAQs) document regarding changes made to the Medicaid continuous enrollment condition under the Families First Coronavirus Response Act (FFCRA) by the Consolidated Appropriations Act 2023 (CAA, 2023). Key topics addressed in the FAQs include questions relating to the CAA, 2023 returned mail condition for states claiming the increased FMAP available under the FFCRA, reestablishment of premiums in Medicaid and CHIP, renewal requirements for individuals who receive Social Security Income, and Medicaid and CHIP agency capacity to share beneficiary data with enrolled providers to support renewals.
These FAQs clarify other CMS guidance most recently released in the January 5, 2023 CMCS Informational Bulletin and January 26, 2023 State Health Official letter #23-002.
Background
On Thursday, December 29, 2022, Congress enacted the Consolidated Appropriations Act, 2023 (CAA, 2023). CAA, 2023 includes various Medicaid and Children’s Health Insurance Program (CHIP) provisions, including significant changes to the continuous enrollment condition at section 6008(b)(3) of the Families First Coronavirus Response Act (FFCRA) that took effect April 1, 2023. Under this section of the FFCRA, states claiming a temporary 6.2 percentage point increase in the Federal Medical Assistance Percentage (FMAP) have been unable to terminate enrollment for most individuals enrolled in Medicaid as of March 18, 2020, as a condition of receiving the temporary FMAP increase. Currently, states must, over time, return to normal eligibility and enrollment operations. States will have up to 12 months to initiate, and 14 months to complete, a renewal for all individuals enrolled in Medicaid, CHIP, and the Basic Health Program (BHP) following the end of the continuous enrollment condition— this process is commonly referred to as “unwinding”.
Under the Consolidated Appropriations Act 2023 (CAA, 2023) expiration of the continuous enrollment condition and receipt of the temporary FMAP increase will no longer be linked to the end of the Covid-19 public health emergency. The continuous enrollment condition ended on March 31, 2023. Beginning April 1, 2023, the FFCRA’s temporary FMAP increase will be gradually reduced and phased down and will end on December 31, 2023. Additionally, as of April 1, 2023, states have been able to terminate Medicaid enrollment for individuals no longer eligible.
Medicaid Unwinding and UIOs
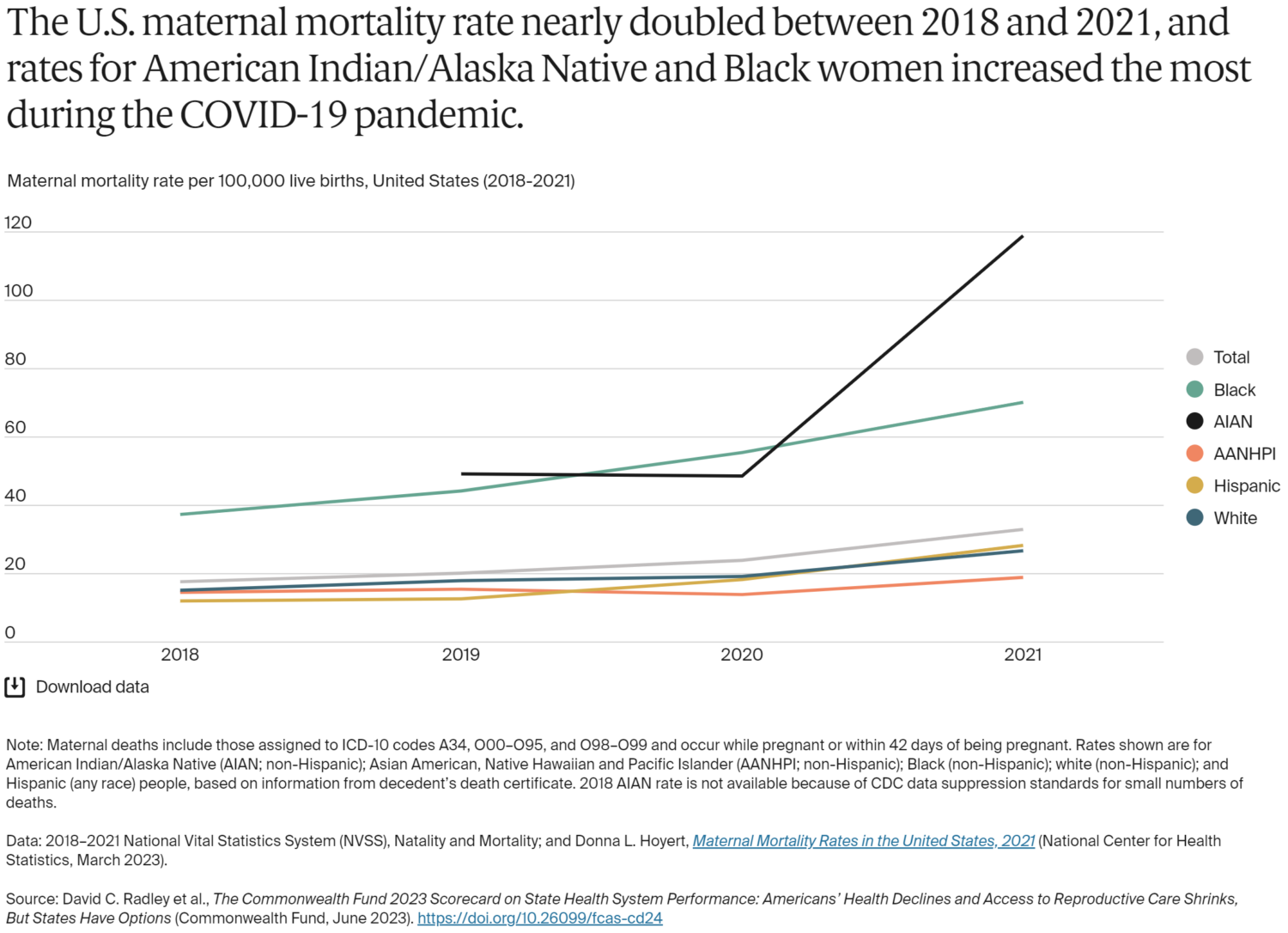
During this unwinding, 12% of all AI/AN children and 6% of all AI/AN adults nationwide are expected to lose CHIP or Medicaid coverage. Urban Indian Organization (UIO) Medicaid beneficiaries may lose their Medicaid coverage as result of the unwinding. The National Council of Urban Indian Health (NCUIH) is helping to mitigate this. It released a Medicaid unwinding toolkit for UIOs in December 2022. On April 24, 2023, NCUIH, in collaboration with the Asian & Pacific Islander American Health Forum, the Coalition on Human Needs, The Leadership Conference on Civil and Human Rights, the National Association for the Advancement of Colored People, National Urban League, Protect Our Care, UnidosUS and 220 other organizations, sent a letter to the Department of Health and Human Services (HHS) Secretary Xavier Becerra. In it, the coalition of organizations called on the Administration to use the full extent of its authorities to safeguard Medicaid coverage and outlined specific steps the Administration can take to avoid wrongful terminations.
See NCUIH’s COVID-19 Public Health Emergency Medicaid Unwinding Toolkit for more information on Medicaid unwinding, its impact on UIO Medicaid beneficiaries and additional resources: https://ncuih.org/2022/12/05/resource-covid-19-public-health-emergency-medicaid-unwinding-toolkit-released/.