Urban Indian Health Policy Updates
February is almost over. Here’s what you missed, and a look ahead!
1 Big Thing: The National Congress of American Indians Honors Partnership with NCUIH

The National Congress of American Indians (NCAI) President Fawn Sharp and Executive Director Larry Wright honor NCUIH President Sonya Tetnowski and CEO Francys Crevier at their Executive Council Winter Session (ECWS) 2023.
Last week, NCAI hosted a Special Recognition Ceremony for Indian Health Care Warriors where NCUIH was honored alongside the National Indian Health Board for our joint effort in securing advance appropriations for the Indian Health Service.
NCUIH was also invited to present at the NCAI’s Executive Council Winter Session before the general assembly. President Tetnowski highlighted NCUIH’s work for improving veterans’ health and celebrated our longtime partnership with NCAI.
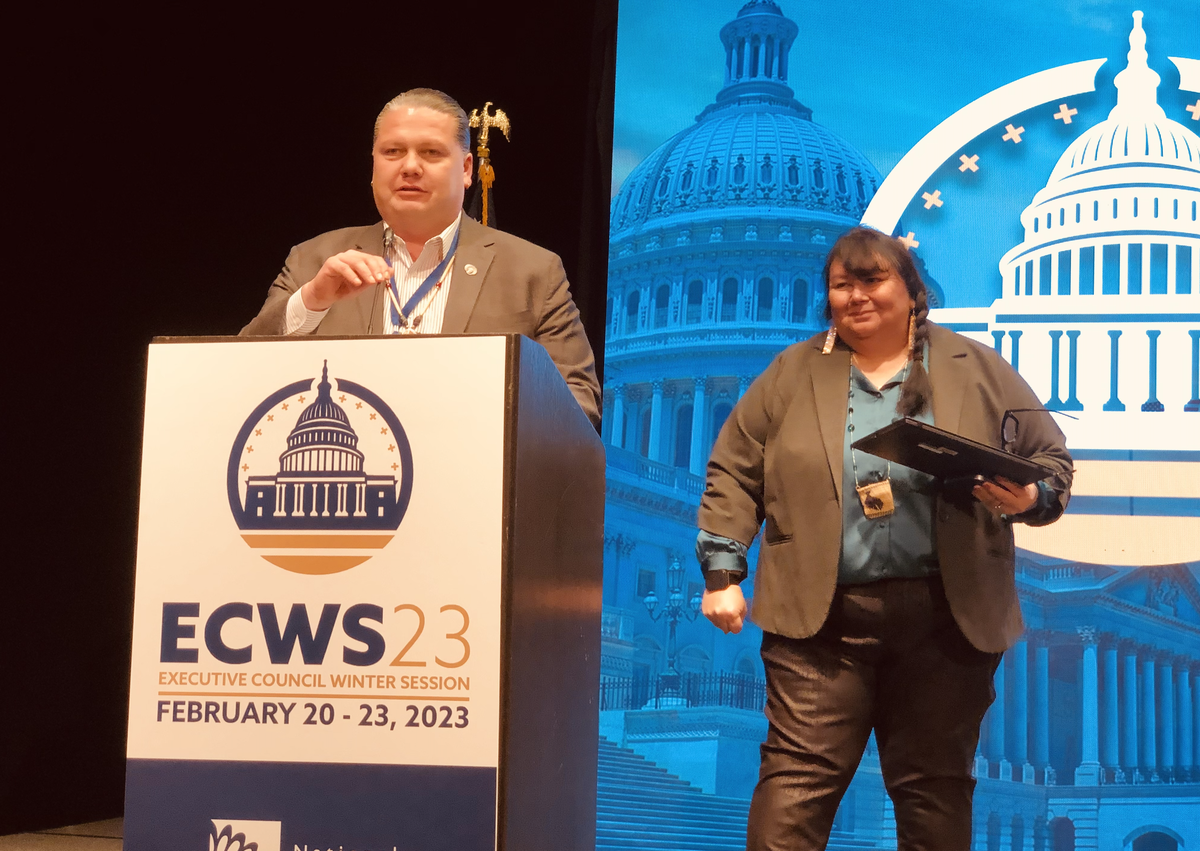
President Tetnowski presents at ECWS.
Why it matters: Inter-organizational efforts are critical for addressing complex issues that require collaboration across multiple sectors and stakeholders. When organizations work together, we can pool resources, expertise, and knowledge to achieve a more significant impact than any one organization could achieve alone. By leveraging the strengths and capabilities of different organizations, inter-organizational efforts can drive innovation and create more sustainable solutions and outcomes for American Indians and Alaska Natives (AI/ANs).

NCUIH team at NCAI Executive Council Winter Session.

NCUIH team at the 2023 State of Indian Nations.
Urban Indian Leaders and NCUIH Attend Budget Formulation

NCUIH at 2023 National Tribal Budget Formulation Workgroup Session.
The Indian Health Service held the National Tribal Budget Formulation Workgroup Session on February 13 and 14 in Washington, DC.
Did you know?: As part of the trust responsibility to provide health care to all American Indians and Alaska Natives, Tribal leaders present their funding needs each year to the Secretary of the Department of Health and Human Services (HHS) and the Director of the Office of Management and Budget.
Why it matters: The recommendations are formed through the Tribal Budget Formulation Work Group (TBFWG) and serve as a framework for the Administration in setting budget amounts for their annual requests to Congress. This process ensures the federal government has the resources to provide health care to all AI/ANs in fulfillment of the trust responsibility.
Save the Date – HHS Annual Tribal Budget Consultation Coming on April 18-19, 2023: The Annual Tribal Budget Consultation provides a forum for Tribes to collectively share their views and priorities with HHS officials on national health and human services funding priorities and make recommendations on HHS’s FY 2025 budget request. This year’s consultation will occur in-person at the Hubert H. Humphrey Building in Washington, D.C. Please see this Dear Tribal Leader Letter for more.
Tribal Leaders Highlight Need for Increased Urban Indian Health Funding in Fiscal Year 2025 IHS Budget Requests
On January 25-26, IHS held its annual Area Report Presentations Webinar for FY 2025 where Tribal leaders from all 12 IHS Areas and leaders from Native organizations, including the NCUIH, presented on their budget requests.
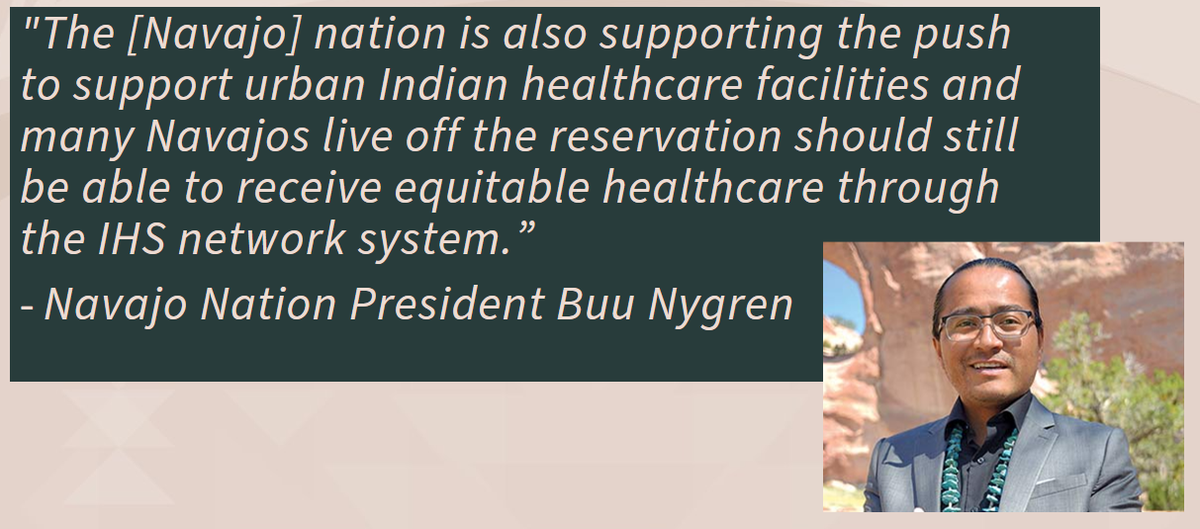
What they’re saying: Many Tribal leaders emphasized the need to increase funding and resources for urban Indian health in the FY2025 budget. Navajo Nation President Buu Nygren stated: “The [Navajo] nation is also supporting the push to support urban Indian healthcare facilities and many Navajos live off the reservation should still be able to receive equitable healthcare through the IHS network system.”
[Read more: Tribal Leaders Highlight Need for Increased Urban Indian Health Funding in Fiscal Year 2025 IHS Budget Requests]
NCUIH Board of Directors Meets with IHS Director Roselyn Tso

IHS Director Roselyn Tso and NCUIH Board President, Sonya Tetnowski
This month, Director Roselyn Tso joined the quarterly NCUIH Board Meeting where she spent time providing updates on key issues at the Indian Health Service and discussing the new IHS 2023 Workplan.
NCUIH to Testify before Congress at Tribal Public Witness Day Next Week

NCUIH’s CEO Francys Crevier will testify before the House Interior Appropriations Subcommittee for American Indian and Alaska Native Public Witness Day.
On March 8 and 9, the Committee on Appropriations, Subcommittee on Interior, Environment, and Related Agencies of the House of Representatives will host American Indian and Alaska Native Public Witness Days.
- NCUIH’s CEO Francys Crevier will testify on March 9 at 9:30 AM.
The bottom line: Congress hosts American Indian and Alaska Native Public Witness Days to hear from stakeholders in Indian Country about budget needs. NCUIH will discuss the need for resources to support access to health care for urban Native communities in its testimony.
More information to follow next week.
Bipartisan Urban Indian Health Confer Act Reintroduced

On February 15, 2023, Senators Tina Smith (D-MN) and Markwayne Mullin (R-OK) re-introduced the Urban Indian Health Confer Act (S.460)
- This is part of an ongoing effort to rectify longstanding parity issues within the Indian health system.
Why it matters: The legislation would require agencies and offices within the U.S. Department of Health and Human Services (HHS) to confer with UIOs on policies and initiatives related to healthcare for urban Native communities.

Go deeper: NCUIH worked closely with the Senators on this bill which was originally introduced in May 2022 as S. 4323 by Sen. Smith, as well as with Representative Raúl Grijalva (D-AZ-7) on the House companion bill (H.R. 630), which was recently re-introduced on January, 30, 2023.
New Report on COVID Funds and Native Orgs, New FMAP Guidance and More Federal Updates
- GAO Report Finds that Tribes and Native Organizations Faced Barriers to Accessing Federal COVID-19 Relief Funds Due to Administrative Burdens
- NCUIH Advocacy Results in New Guidance from HHS on 100% FMAP for Urban Indian Organizations
- Centers for Medicare and Medicaid Services (CMS), issued guidance that creates an easier path to specialty care for Medicaid and CHIP beneficiaries..
- CMS Director Publishes State Health Official Letter #23-002 Issuing Guidance to States on Medicaid Continuous Enrollment Condition Changes
NCUIH Monitoring Supreme Court Case: Lac du Flambeau Band of Lake Superior Chippewa Indians v. Coughlin

The Lac du Flambeau Band of Lake Superior Chippewa Indians v. Coughlin case before the Supreme Court centers on the question of tribal sovereign immunity and its applicability to state regulatory actions. The tribe contends that they are immune from state regulatory action because of their sovereign status, while the state maintains that it has a legitimate interest in regulating tribal activities that affect public health and safety. The Supreme Court’s decision, in this case, could have significant implications for the balance of power between states and tribes and the scope of tribal sovereignty in the United States.
The Issue at Hand: Whether the Bankruptcy code “unequivocally” abrogates Tribal sovereign immunity by stating the Code applies to “other domestic and international governments” without specifically listing Tribes.
How would this apply to UIOs?
- How the Court decides this case has the potential to weaken the statutory language necessary to abrogate Tribal sovereignty. This case is more attenuated to UIOs specifically but will have ramifications throughout the federal Indian law space.
- Native American Rights Fund has an amicus workgroup for this case, and NCUIH is attending.
What’s next: Appeal from the 1st Circuit, Cert. Granted Jan. 13, 2023, Oral Argument scheduled for April 24th, 2023- expected at 1 pm.
Upcoming Events and Important Dates
- March 3 – Comment Deadline for Office of the Assistant Secretary for Health Strengthening Primary Health Care
- March 8 – House Appropriations Committee American Indian and Alaska Native Public Witness Days
- March 9 – NCUIH Testifying at House Appropriations Committee American Indian and Alaska Native Public Witness Day
- March 8-9 - IHS Tribal Self-Governance Advisory Committee Meeting (TSGAC)
- March 15 – NCUIH Monthly Policy Workgroup
One last thing: NCUIH Early Bird Registration Ends March 15

Early Bird Registration is now open for our 2023 Annual Conference!
Our conference will be held May 15-18, 2023 with the option of joining us in person in Washington, D.C., or virtually. This year’s theme is Honoring Our Ancestors & Preparing for the Next Seven Generations: NCUIH Celebrates 25 Years of Health Leadership. (Register Here)
Note: Early Bird Registration ends March 15.
Thank you for all your hard work and advocacy!