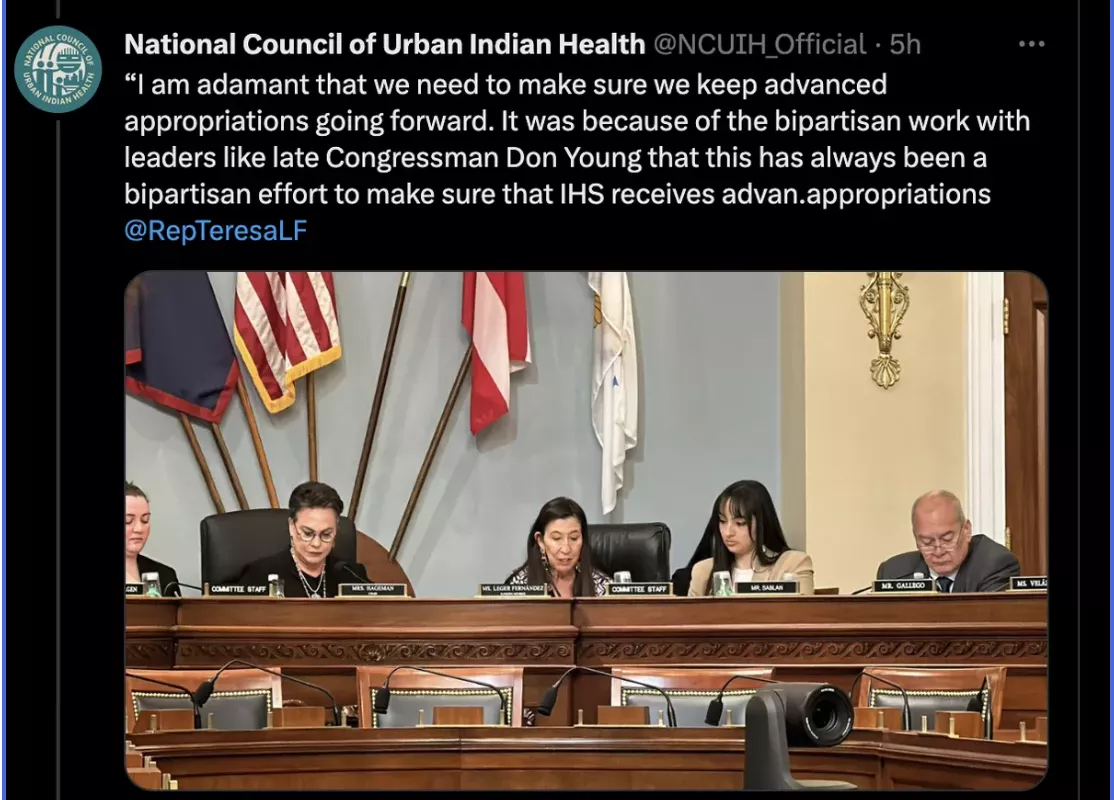
The National Council of Urban Indian Health (NCUIH) Board Member and Chief Operations Officer (COO) of the NATIVE Project, Maureen Rosette (Chippewa Cree Nation), testified before the House Natural Resources Subcommittee on Indian and Insular Affairs oversight hearing titled “Challenges and Opportunities for Improving Healthcare Delivery in Tribal Communities.”
NCUIH Testifies at Congressional Hearing on Tribal Healthcare Delivery and Funding for IHS
NCUIH Board Member and COO of the NATIVE Project, Maureen Rosette (Chippewa Cree Nation), testifies before the House Natural Resources Subcommittee on Indian and Insular Affairs.
On Wednesday, March 29, NCUIH Board Member and NATIVE Project COO, Maureen Rosette, testified before the Subcommittee on Indian and Insular Affairs in their oversight hearing titled “Challenges and Opportunities for Improving Healthcare Delivery in Tribal Communities.”
Additional witnesses included: Ms. Janet Alkire, Board Member
of the National Indian Health Board, Ms. Jerilyn Church, Executive Director of the Great Plains Tribal Leaders Health Board, and Ms. Laura Platero, Executive Director of the Northwest Portland Area Health Board.
What they’re saying:
In her opening remarks, Chairwoman Harriett Hageman (R-WY- AL) reaffirmed the trust and treaty obligation to Native health care, stating that “the federal government has taken upon itself to provide for the care of American Indians and Alaska Natives.”
Rosette emphasized the importance of the Indian Health Service (IHS) and urban Indian organizations (UIOs) to the Indian health system in providing health care to Native people.
“I lived and grew up on my reservation and I was a consumer of my own Tribally-operated health program at the age of 28. I moved to Spokane to go to law school. I had no health insurance. I had two little kids, a three-year-old and a five-year-old and we had no health insurance. At the time, if NATIVE Project had medical services, we would at least had access to health care, but we didn’t at the time. I just hoped and prayed that none of us got sick. Now, I have insurance and can go anywhere I want, but our family has chosen to be consumers of NATIVE Project because of the excellent healthcare we get there. And it’s culturally appropriate, that’s what we want. Today, there are 41 UIOs, which are a fundamental and necessary component of the Indian health system, and we work hand in hand with IHS to help provide the resources necessary to provide healthcare to Native people.”
-Maureen Rosette, NCUIH Board Member and NATIVE Project COO
The importance of care for Native people by Native people was also reiterated in the hearing including by Ms. Laura Platero:
“While American Indian and Alaska Native people were disproportionality impacted by COVID-19, due to underlying health disparities and the lack of infrastructure in many communities, Tribal innovation and response to COVID prevailed. When Tribes are given the resources and the control of those resources, they know how to respond to meet the needs of their community.”
-Laura Platero, Executive Director, Northwest Portland Area Indian Health Board
The bottom line: The IHS including UIOs are a critical resource for Native people to access healthcare services.
Proposed Cuts to IHS Funding Risks Native Lives
Witnesses and Members of Congress at hearing on Indian Health Service oversight.
Rosette, along with fellow witnesses, provided valuable insight into the realities that Native communities experience at home in their call for more reliable funding for IHS.
Addressing Challenges: The shortage of healthcare professionals and facilities in rural and urban areas, coupled with the difficulty recruiting and retaining them, makes it difficult for patients to access quality healthcare. The lack of adequate resources, poor infrastructure, and low salaries have resulted in a shortage of healthcare professionals in these areas. Native leaders spoke about the importance of supporting Native healthcare administrators in their effort to be innovative and creative care providers for their people.
“Congress must live up to its treaty commitments, bring IHS facilities to modern standards, and increase IHS funding. After this hearing, I will return home to our financially starved IHS hospital covered in snow and running on boiler heat in below-freezing temperatures. I will give all my time and energy to help my people in need, working my vision for a new medical facility… I will be waiting for this subcommittee and Congress to finally take action, Congress must pay its overdue debts and provide American Indians and Alaska Natives the healthcare we deserve and the healthcare we were promised.”
-Janet Alkire, National Indian Health Board
Advanced funding for IHS is needed to provide stable and predictable funding to ensure the continuity of care for American Indian and Alaska Native people.
“Advance Appropriations will now allow IHS to make long-term cost-saving purchases and minimize the administrative burdens for the agency and UIOs. It will also improve accountability and increase staff recruitment and retention at IHS. When IHS distributes its funding on time, our UIOs can pay their doctors and providers- giving Native people the access to care and services they need to be thriving communities.”
-Maureen Rosette, NCUIH Board Member and NATIVE Project COO
What they’re saying:
“GOP proposed cuts to IHS would have to reduce outpatient services by nearly 1.6 million visits. 1.6 million visits will go away. Dental visits would be reduced by 120,000, mental health visits by nearly 90,000 and outpatient services by 4,000.”
Next Steps: The Committee is expected to review the testimony as they propose oversight legislation related to the Indian Health Service this year. NCUIH will continue to advocate for full and flexible funding for the Indian Health Service.
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501NCUIHhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngNCUIH2023-03-31 16:06:012023-04-05 10:58:20NCUIH Testifies Before House Oversight Committee on Improving Healthcare Delivery for Native People
On February 15-16, 2023, the National Council of Urban Indian Health (NUCIH) Federal Relations Manager, Alexandra Payan, represented NCUIH at the Substance Abuse and Mental Health Services Administration’s (SAMHSA) American Indian and Alaska Native (AI/AN) Veterans Expert Panel Discussion. The purpose of this two-day meeting was to have a collaborative conversation around the development of a virtual training tool related to AI/AN military and veteran suicide prevention. The proposed tool will be available for states, territories, and communities to use as they work to implement their efforts. NCUIH was invited to participate in the Expert Panel Discussion to provide insight on the unique needs of AI/AN veterans who reside in urban areas.
Expert Panel’s Work to Support the Governor’s Challenge
The Expert Panel Discussion was an opportunity to ensure broad representation of AI/AN veterans in the Governor’s Challenge to Prevent Suicide Among Service Members, Veterans, and their Families (Governor’s Challenge). Through collaboration with the VA, SAMHSA and SAMHSA’s SMVF Technical Assistance Center, the Governor’s Challenge seeks to provide a forum for teams to consider how existing policies, practices, infrastructure, and resources influence the effectiveness of the systems that support SMVF. Teams develop state and territory-wide plans based on a comprehensive public health approach and the National Strategy for Preventing Veteran Suicide (National Strategy). During the Expert Panel Discussion, the team engaged in initial steps to develop a virtual toolkit aimed at addressing suicide in AI/AN veteran communities to supplement the Governor’s Challenge. Once created, the virtual toolkit will serve as instruments of change, providing a best-practice public health model that demonstrates meaningful results in suicide prevention for AI/AN veterans.
Urban Indian Organizations and Native Veteran Support
Sadly, AI/AN veterans have a higher prevalence of mental health disorders compared with White veterans and among all veterans the prevalence of suicidal ideation is highest for those reporting a diagnosis of depression, anxiety, or post-traumatic stress disorder. While there is limited data and research on suicide among AI/AN veterans, the 2020 National Veteran Suicide Prevention Annual Report documents growing AI/AN veteran suicide rates from 2005-2018.
UIOs are essential partners in serving AI/AN veterans and reducing AI/AN veteran suicides. UIOs are critical in improving care and access to services for AI/AN veterans because of their deep ties to the AI/AN community in urban areas. UIOs currently serve seven of the ten urban areas with the largest AI/AN veteran populations, including Phoenix, Arizona; Los Angeles, California; Seattle, Washington; Dallas, Texas; Oklahoma City, Oklahoma; New York City, New York; and Chicago, Illinois. Many AI/AN veterans prefer to receive care at IHS facilities, or may only have access to an IHS, Tribal, or UIO facility.
UIOs are uniquely positioned to assist agencies, such as the VA, SAMHSA, and HHS, in improving health care access for AI/AN people. Several UIOs already provide mental health and substance abuse disorder services and all UIOs provide numerous other social and community services to AI/ANs living in urban areas. NCUIH looks forward to continuing to work with SAMHSA, VA, and other agencies to improve the quality of care available to Native veterans in urban areas.
NCUIH’s work with the VA and Native Veterans in Urban Areas
NCUIH continues to work on behalf of Native veterans living in urban areas to ensure that they have access to the high-quality, culturally competent care the country owes to them for their military service and as a result of the trust responsibility.
For more information on NCUIH’s efforts please visit:
On Wednesday, March 29 at 10:00 a.m. EDT, NCUIH Board Member and Chief Operations Officer of the NATIVE Project, Maureen Rosette (Chippewa Cree Nation), will be testifying before the House Natural Resources Subcommittee on Indian and Insular Affairs oversight hearing titled “Challenges and Opportunities for Improving Healthcare Delivery in Tribal Communities.” During the hearing, NCUIH will advocate for stable and reliable funding for IHS by maintaining advance appropriations to improve healthcare delivery to American Indians and Alaska Natives, while also highlighting the important work UIOs are doing to provide care to their communities.
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501NCUIHhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngNCUIH2023-03-28 11:00:012023-03-28 11:00:01NCUIH to Testify before the House Natural Resources Subcommittee on Indian and Insular Affairs
Greetings and Happy Spring! In this month’s newsletter, we bring you important updates and information regarding our latest developments and initiatives within the Urban Indian Health Community.
1 Big Thing: Sec Deb Haaland Hosts MMIP Commission Including NCUIH President
Secretary Deb Haaland alongside members of the Not Invisible Act Commission.
The National Council of Urban Indian Health (NCUIH) President, Sonya Tetnowski (Makah), joined Secretary of the Interior Deb Haaland for a meeting as a member of the Not Invisible Act Commission.
Why it matters: The Commission aims to combat the epidemic of missing and murdered American Indians and Alaska Natives (AI/ANs) and features a diverse group of experts and stakeholders who are tasked with conducting a comprehensive study of the issue and making recommendations to the federal government on how to address it. The Commission’s work is ongoing, and it represents an important step towards addressing this critical issue and ensuring justice and safety for American Indian and Alaska Native communities.
“A lack of urgency, transparency, and coordination has hampered our country’s efforts to combat violence against American Indian and Alaska Native people. In partnership with the Justice Department and with extensive engagement with Tribes and other stakeholders, the Interior Department is marshaling our resources to finally address the crisis of violence against Indigenous peoples,” —Secretary Deb Haaland.
President Biden’s FY 2024 Budget Includes Increased Investment in the Indian Health Service
President Biden delivering his Budgetary speech with a quote from IHS Director Tso.
On March 9, 2023, the President released the annual budget proposal for FY 2024 with commitment that by 2025, the IHS budget would shift from mostly discretionary to all mandatory funding as a long-term solution. The Administration also continues to prioritize advance appropriations for IHS until this solution is enacted.
Urban Indian Health:$115 Million for an increase of $25 million or 27% above FY 2023 enacted and $858.6 million less than requested by the TBFWG.
Reauthorizes and Increases Funding for the Special Diabetes Program for Indians: The budget proposes to reauthorize the Special Diabetes Program for Indians and provide $250 million in FY 2024, $260 million in FY 2025, and $270 million in FY 2026 in new mandatory funding. SDPI’s current authorization is set to expire on September 30, 2023.
Proposes New Program to Increase Public Health Capacity and Infrastructure: The budget also proposes new funding of $150 million in FY 2025 to address public health capacity and infrastructure needs in Indian Country. This funding would support an innovative hub-and-spoke model to address local public health needs in partnership with tribes and UIOs.
NCUIH CEO, Francys Crevier delivering testimony at Witness Day.
On March 9, 2023, NCUIH CEO Francys Crevier (Algonquin), testified before the House Interior Appropriations Subcommittee as part of AI/AN Public Witness Days regarding FY 2024 funding for the IHS. NCUIH was invited to testify on the critical health needs of AI/ANs living in urban areas and requested full funding for IHS.
“Native people deserve full, healthy lives. We cannot continue to rely on short-term solutions that only address the symptoms of the problem. We ask for full funding for IHS and the urban Indian health line item. Make advance appropriations and 100% FMAP for UIOs permanent. Protect us from sequestration now,” —Francys Crevier (Algonquin), NCUIH CEO.
NCUIH Presents Before the American Academy of Pediatrics Committee on Native American Child Health
NCUIH’s Director of Congressional Relations, Lycia Maddocks (Quechan), and AAP Chairperson, Allison Empey MD, FAAP.
NCUIH’s Director of Congressional Relations, Lycia Maddocks, recently presented before the American Academy of Pediatrics (AAP) Committee on Native American Child Health (CONACH) to discuss NCUIH’s policy priorities and efforts in the Native child health space.
Why it matters: The presentation was an opportunity for NCUIH to showcase its initiatives aimed at improving the health outcomes of AI/AN children, including efforts to increase access to healthcare services, improve health education, and address disparities in care. Maddocks’ presentation is a part of NCUIH’s ongoing advocacy efforts to promote policies and programs that support the health and well-being of urban Indian communities. By engaging with organizations like the AAP, NCUIH can work to ensure that the unique healthcare needs of AI/AN children are being addressed and that their voices are being heard.
Policy and Communications Vice President, Meredith Raimondi, alongside AAP panelists.
On February 28, Meredith Raimondi, the Vice President of Policy and Communications at NCUIH, participated in a panel discussion hosted by AAP to discuss the importance of advance appropriations for the Indian Health Service (IHS), which was included in the Fiscal Year (FY) 2023 spending bill.
What Happened: NCUIH spoke to the importance of advance appropriations and how it would provide funding for IHS programs in advance of the fiscal year, giving urban Indian organizations (UIOs) greater stability in their budgeting and planning processes.
Did you know?: Prior to the inclusion of advance appropriations in the FY2023 spending bill, the Indian healthcare system—including IHS, Tribal facilities, and UIOs—was the only major federal healthcare provider funded through annual appropriations. Advance appropriations will stabilize IHS funding and allow for long-term planning by insulating Indian healthcare providers from government shutdowns and continuing resolutions. AI/ANs will no longer be uniquely at risk of death or serious harm during delays in an FY 2024 funding agreement.
NCUIH Participates in SAMHSA’s Native Veterans Expert Panel Discussion and Visits Oklahoma City Indian Clinic
Captain Karen Hearod, Director of the Office of Tribal Affairs and Policy, SAMHSA and NCUIH’s Federal Relations Manager, Alexandra Payan.
NCUIH Federal Relations Manager, Alexandra Payan, participated in the Substance Abuse and Mental Health Services Administration’s (SAMHSA) AI/AN Veterans Expert Panel Discussion on the development of a virtual training tool related to AI/AN military and veteran suicide prevention and provided insight on the unique needs of Native veterans who reside in urban areas.
OKCIC Vice-President of Policy, Diabetes and Prevention, Michelle Dennison and NCUIH’s Federal Relations Manager, Alexandra Payan.
Ms. Payan also visited the Oklahoma City Indian Clinic and had the opportunity to meet with staff and learn more about the clinic’s programs and services, as well as the challenges and opportunities facing UIOs in Oklahoma and across the country. By gaining a firsthand understanding of the issues and needs facing UIOs, NCUIH can better advocate for policies and programs that support their work and ensure access to high-quality, culturally competent healthcare for AI/AN communities. Read more about Ms. Payan’s visit here.
NCUIH’s 2022 Policy Assessment Now Available
NCUIH’s 2022 Policy Assessment can be accessed on the NCUIH website.
NCUIH hosted five focus groups to identify UIO policy priorities for 2023 and to evaluate NCUIH’s progress toward achieving goals from previous years.
The Assessment covers a wide range of issues related to AI/AN health and well-being, including healthcare access and funding, mental health, substance abuse, and social determinants of health.
The assessment also includes an analysis of the policy landscape and the impact of recent policy changes on AI/AN communities.
Overall, the assessment highlights both the progress that has been made in improving AI/AN health outcomes and the ongoing challenges that remain.
It provides a valuable resource for policymakers, advocates, and other stakeholders who are working to advance policies and programs that support the health and well-being of AI/AN communities.
The big picture: IHS is developing and implementing a work plan to identify, assess, report, and manage enterprise-level risks that impact the IHS environment. In support of the agency’s enterprise risk management efforts, the goal of the 2023 Agency Work Plan is to make an immediate impact on the Indian health system in alignment with the IHS mission and Strategic Plan.
IHS released a letter to Urban Indian Organization Leaders to clarify use of funds requirements arising from the FY 2022 Infrastructure Study.
The bottom line: In the letter, IHS clarifies additional $800,696 in funding allocated in the Consolidated Appropriations Act, 2022 is not intended for UIO infrastructure study activities, emphasizing that “…the joint explanatory statement accompanying the Consolidated Appropriations Act, 2022, does not mean Congress intends to allocate additional funding for UIO Infrastructure Activities. Instead, Congress intends to ensure that the additional funding provided remains in the Direct Operations accounts of IHS management use.” IHS notes that this aligns with UIO Confer recommendations to avoid using the funding for any additional UIO Infrastructure Study activities.
NCUIH-Endorsed Bridging Agency Data Gaps & Ensuring Safety (BADGES) for Native Communities Act Reintroduced
On March 1, 2023, Representatives Ruben Gallego (D-AZ), Dan Newhouse (R-WA), and Sharice Davids (D-KS) reintroduced the BADGES for Native Communities Act.
The bill addresses federal inefficiencies that hurt Bureau of Indian Affairs law enforcement recruitment and retention, increases the effectiveness of federal missing persons resources, and gives resources to Tribes and states to combat the crisis of missing and murdered Indigenous women and girls.
“This legislation is one way to help bring justice and closure to Native families and communities and hopefully will make it so fewer Native families have to suffer this terrible burden in the future. We must continue to advocate for policies that prioritize the safety and wellbeing of Indigenous communities, and the passage of this Act is a critical step in that direction,” —Francys Crevier (Algonquin), NCUIH CEO.
NCUIH Monitoring Supreme Court Case: Department of Interior v. Navajo Nation
The United States Supreme Court heard arguments regarding Navajo water rights and the US government’s obligations to the Tribe.
The Issue at Hand: The case concerns whether the US government is required to compensate the Navajo Nation for the use of its water by the San Juan River, which is a crucial source of water for the Tribe. The Navajo Nation argues that the US government has not fulfilled its responsibilities under the Winters Doctrine, which grants Native American tribes the right to use water on their reservations for necessary purposes. The government, on the other hand, contends that it has already met its obligations under the doctrine and that the Navajo Nation is not entitled to additional compensation.
What’s Next: Following Monday’s hearing, the next step in the Navajo Nation water rights case is for the court to issue a ruling, which is expected to occur later this year.
Why it matters: The decision could have significant implications for tribal water rights and the government’s obligation to Native American tribes. If the court rules in favor of the Navajo Nation, it could set a precedent for other tribes seeking compensation for the use of their water resources. On the other hand, if the court rules in favor of the government, it could limit the extent of the federal government’s responsibility to Native American tribes under the Winters Doctrine. Regardless of the outcome, the case is likely to have a significant impact on the relationship between the US government and Native American tribes and could shape policy decisions for years to come.
March 23- NCUIH is submitting written testimony to the House Appropriations Subcommittee on Labor, Health and Human Services and Education on urban Indian health priorities.
March 24- NCUIH working with UIOs and submitting budget requests to Congress.
April 7 – Comment deadline for IHS on HIT Modernization: Preparing for Change
April 24 – Comment deadline for IHS on Executive Order 14001 – Access to Federal Medical Supplies
May – HHS Budget Testimony
ICYMI:
NCUIH met with the White House Council on Native American Affairs (WHCNAA) on Feb. 22 to further discuss the Homeless Veteran Initiative that was announced at the White House Tribal Nations Summit.
NCUIH has conducted four (4) UIO interviews to gather information regarding Primary Care Case Management programs (PCCMs) and Indian Managed Care Entities (IMCEs) for this year’s NORC report.
Medicaid and Health Reform Policy Committee (MMPC) Face-to-Face Virtual Meeting was held on March 14.
Tribal Leaders Diabetes Committee (TLDC) Quarterly meeting was held on March 14-15.
CMS Tribal Technical Advisory Group (TTAG) held it’s Face-to-Face meeting with CMS leadership on Mar. 15-16.
One last thing: NCUIH Annual Conference Registration and Award Nominations
Our conference will be held May 15-18, 2023 with the option of joining us in-person in Washington, D.C., or virtually. This year’s theme is Honoring Our Ancestors & Preparing for the Next Seven Generations: NCUIH Celebrates 25 Years of Health Leadership. (Register Here)
This year’s theme, “Honoring Our Ancestors & Preparing for the Next Seven Generations: NCUIH Celebrates 25 Years of Health Leadership,” is a great opportunity to celebrate and recognize the accomplishments of the urban Indian health community.
As part of this celebration, we will be recognizing individuals and organizations that have made significant contributions to the field of urban Indian health. We are pleased to invite you to nominate candidates for the following awards:
1. UIO Staff Member of the Year 2. Local Urban Indian Leadership Award 3. UIO Innovation Award 4. Urban Indian Legacy Award 5. Rising Ally Award 6. National Urban Indian Policy Impact Award 7. Native Veterans Health Ally Award
Please use the linked Asana form to submit your nominations. The form includes instructions on the nomination process and the criteria for each award. Please note that the deadline for nominations is Monday, April 17.
https://ncuih.org/wp-content/uploads/2023-Web-Assets_NCUIH_D356-V2-SM_Policy-Update.png23443125NCUIHhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngNCUIH2023-03-23 10:51:012025-06-10 11:09:32Urban Indian Health Policy Updates
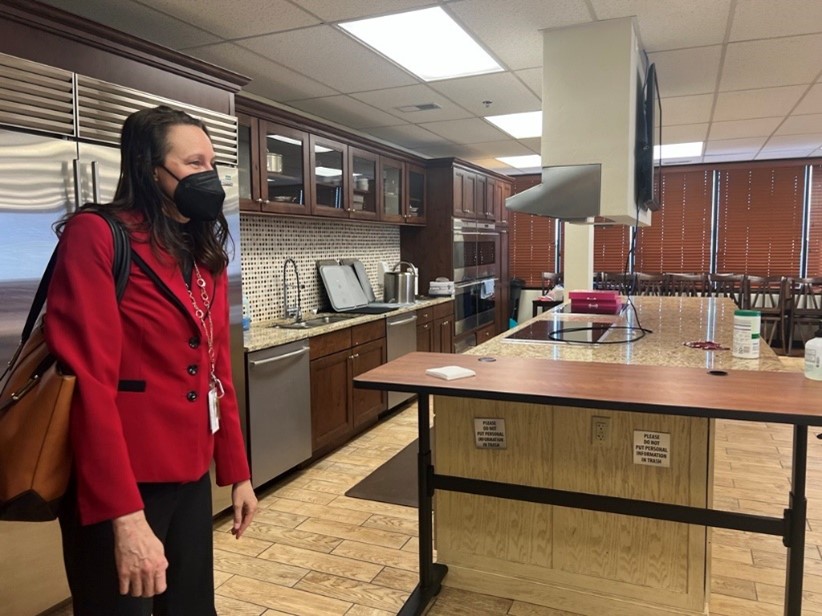
NCUIH’s Federal Relations Manager, Alexandra Payan, recently visited the Oklahoma City Indian Clinic (OKCIC), which has provided extensive health and social services to AI/ANs living in Oklahoma City for almost 50 years. Ms. Payan toured the facilities and met with OKCIC Executive Director, Robyn Sunday-Allen and Vice-President of Policy, Diabetes and Prevention, Michelle Dennison. Ms. Sunday-Allen also serves as Vice-President of NCUIH’s Board of Directors. Ms. Payan and OKCIC leadership discussed upcoming projects for the OKCIC, including breaking ground on the new women’s health and pediatric facility OKCIC purchased last year and continued expansion for the growing facility that serves over 22,000 patients from over 200 federally recognized Tribes each year. During the tour, Ms. Payan was also able to see the facility’s demonstration kitchen where they host classes for all ages through their healthy eating/nutrition program.
NCUIH is excited to see the great work OKCIC is doing for their community and looks forward to the many new projects ahead!
OKCIC’s Demonstration Kitchen
OKCIC’s Michelle Dennison and NCUIH’s Alexandra Payan
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501Alexandra Payanhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngAlexandra Payan2023-03-21 10:33:372023-03-21 10:41:27NCUIH Staff Member Visits Oklahoma City Indian Clinic
On April 5, 2023, Health Resources & Services Administration’s (HRSA) Office of Intergovernmental and External Affairs (IEA) will host a tribal listening session on understanding historical trauma and its impacts on the American Indian/Alaska Native (AI/AN) workforce. HRSA’s goal is to advance tribal health systems and resources, partnering with federal agencies and other organizations to increase access to HRSA programs aimed to advance healthcare. Working with the tribal communities, HRSA aims to increase opportunities to access and optimize the quality and performance of the tribal health system increasing the capacity of Indian Country to respond to the impact of negative health outcomes among AI/AN communities. To help tribal organizations maximize the impact of key government programs, HRSA has prioritized increasing urban Indian health participation in the Health Center Program.
Background
The mission of HRSA IEA is to provide accessibility and awareness of HRSA programs designed to increase healthcare access and address emerging public health issues. HRSA IEA serves as the principal Agency lead on intergovernmental and external affairs, regional operations, and tribal partnerships. HRSA IEA extends the reach of its programs by leveraging knowledge of national and regional contact located in various states, tribes, and territories. HRSA IEA also maintains partnerships across federal, state, and tribal networks to promote Department of Health and Human Services (HHS) policy priorities.
AI/AN Historical Trauma
Historical trauma is the cumulative psychological and emotional wounding across generations. For Tribal nations and the AI/AN community, historical trauma began during the eras of colonization, forced removal, and government sponsored boarding schools aimed to destroy AI/AN people and culture. Today, the impact of historical trauma is manifested in many ways among AI/ANs including high rates of chronic diseases, suicides, domestic violence, alcoholism, and other social problems such as the lack of culturally competent care often leading to poor communication between physicians and patient that increase rick of misdiagnosis and loss of public trust. These ailments are negatively attributed across social determinants of health thereby impairing the ability to readily participate in the workforce.
NCUIH’s Role
NCUIH has advocated extensively for policy related to healing and reconciliation of historical trauma which continues to afflict AI/AN communities. For example, NCUIH endorsed the Truth and Healing Commission on Indian Boarding School Policies in the United States Act. This bill would create a Truth and Healing Commission on Indian Boarding School Polices in the United States where impacts and ongoing effects of Indian Boarding School Policies are examined. The Commission will also provide a space for AI/AN people to speak about their personal experiences in government-run boarding schools and allow them to provide recommendations to the government.
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501Colin Tompsonhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngColin Tompson2023-03-20 16:06:462023-03-20 16:09:44HRSA Hosting Tribal Listening Session Regarding Historical Trauma and its Impact on the American Indian/Alaska Native Workforce
On February 27, 2023, Centers for Medicare & Medicaid Services (CMS) issued a new fact sheet regarding the ending of the federal Public Health Emergency for COVID-19 (PHE). The PHE was declared by the Department of Health and Human Services (HHS) under Section 319 of the Public Health Services Act and is scheduled to expire at the end of the day on May 11, 2023. The fact sheet is intended to provide clarity of the following services for receiving health care at the end of the PHE:
COVID-19 vaccines, testing, and treatments
Telehealth services
Health Care Access: Continuing flexibilities for health care professionals
Inpatient Hospital Care at Home: Expanded hospital capacity by providing inpatient care in a patient’s home.
What Won’t Be Affected
There are significant flexibilities and actions that will not be affected during the transition to the ending of the PHE. HHS is committed to ensuring that COVID-19 vaccines and treatments will be widely accessible to all who need them. There will also be continued access to pathways for emergency use authorizations (EUAs) for COVID-19 products through the Food and Drug Administration (FDA), and telehealth flexibilities will continue to exist for those participating in Medicare or Medicaid.
Medicaid Continuous Enrollment
The continuous enrollment condition for individuals enrolled in Medicaid is no longer linked to the end of the PHE. Under the Families First Coronavirus Response Act, states claiming a temporary 6.2 percentage point increase in the Federal Medical Assistance Percentage (FMAP) have been unable to terminate enrollment for most individuals enrolled in Medicaid as of March 18, 2020, as a condition of receiving the temporary FMAP increase. As part of the Consolidated Appropriations Act, 2023, the continuous enrollment condition will end on March 31, 2023. The temporary FMAP increase will be gradually reduced and phased down beginning April 1, 2023 and will end on December 31, 2023.
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501Colin Tompsonhttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngColin Tompson2023-03-20 14:46:152023-03-20 14:52:18CMS Provides New Fact Sheet Regarding CMS Waivers, Flexibilities, and the Transition Forward from the COVID-19 Public Health Emergency
On March 20, 2023, the National Council of Urban Indian Health (NCUIH) signed on to a Partnership for Medicaid letter to Chair Bernard Sanders and Ranking Member Bill Cassidy of the Senate Committee on Health, Education, Labor, and Pensions (HELP). This letter is in response to the Senate HELP request for information (RFI) following its February hearing on understanding the root causes of our current health care shortages and exploring potential legislative solutions.
The Letter Identifies Drivers of Workforce Shortages:
State provider payment rates are insufficient to achieve the goal of being able to recruit and retain enough providers to serve Medicaid beneficiaries.
Insufficient supply/Increased demand of providers for populations served by the Medicaid program.
The Letter Recommends:
Grants administered by relevant federal agencies such as the Department of Labor (DOL) and the Department of Health and Human Services (HHS) to strengthen the healthcare workforce, including the direct care workforce.
Expand loan repayment programs to include more health workers, especially those who come from disadvantaged backgrounds and/or racial or ethnic minorities.
Ensure broad eligibility for federal programs intended to increase providers in underserved areas.
Safety from Violence for Healthcare Employees (SAVE) Act (H.R. 7961), legislation that would protect caregivers from workplace violence.
Full Letter Text
Dear Chairman Sanders and Ranking Member Cassidy:
The following are part of a nonpartisan, nationwide coalition comprised of organizations representing clinicians, health care providers, safety net plans, and counties dedicated to preserving and improving the Medicaid program. The undersigned organizations appreciate the opportunity to provide comments in response to your request for input from stakeholders to best understand views on the drivers of health care workforce shortages and ideas on potential solutions. In our view, workforce shortages, especially those seen in providers and professionals struggling to care for the Medicaid population, stem from insufficient payment rates, insufficient supply of providers, and increased demand for particular services most acutely in urban and rural underserved areas. These challenges impact the ability of health care providers and plans to provide needed services to our nation’s most vulnerable: low-income children, pregnant individuals, parents, individuals with disabilities, seniors, and other adult Medicaid beneficiaries across the country. Below, we provide recommendations for specific policy solutions within your Committee’s jurisdiction that would start to address some of these issues. We hope to continue working with the HELP Committee as you begin to shape these policy solutions into actionable legislation.
Drivers of Workforce Shortages
State provider payment rates are insufficient to achieve the goal of being able to recruit and retain enough providers to serve Medicaid beneficiaries. While Federal law mandates that state Medicaid payments be “sufficient to enlist enough providers so that care and services are available under the [state] plan,”existing Federal regulations fail to adequately measure and enforce adequate payment rates. As such, Medicaid has notably low reimbursement rates, that are often much lower than Medicare payment rates, and at times lower than the actual cost of providing care to Medicaid patients. This makes it more difficult for the program to enlist a sufficient number of providers who can meet patient demand, and thus negatively impacts access to care for Medicaid beneficiaries, who are disproportionately people of color.
Insufficient supply of providers for populations served by the Medicaid program. Even before the pandemic, many types of providers and clinicians, including the longterm care community, behavioral health providers, and primary care providers as well as clinicians, increasingly experienced worsening workforce issues, and the COVID-19 pandemic only accelerated this decline. For a variety of reasons, including cost of education, not enough people are pursuing careers in these important fields.
Increased demand for provider types serving the Medicaid program. Due to COVID-19 and other factors, certain types of providers are experiencing ongoing surges in demand, likely to continue for the foreseeable future. For example, our aging population will continue to significantly increase demand for long-term care services, for which Medicaid is the primary payer.More than two-thirds of older adults will need some personal assistance in their daily lives, and nearly half will have a high enough level of need that they will be eligible for private long-term care insurance or Medicaid at some point in their lives. Further, the COVID-19 pandemic has exacerbated an already significant mental health crisis in this country, increasing demand for mental health services and further stretching the existing capacity of mental health providers serving the Medicaid population.
Recommendations
Grants administered by relevant federal agencies such as the Department of Labor (DOL) and the Department of Health and Human Services (HHS) to strengthen the healthcare workforce, including the direct care workforce.
The Committee should consider legislation that would authorize increased funding to relevant federal agencies within its jurisdiction to increase investments that support the recruitment, training, retention, and professional development of a diverse clinical and non-clinical workforce.
For example, the legislation can authorize funding to DOL to award grants to health care entities in health professional shortage areas to support the hiring, training, and retention of healthcare workers, including direct care workers.
The legislation could also authorize funding to HRSA to carry out grants for health care entities for pilot demonstrations to enhance the skills of healthcare workers including direct care workers mental health professionals and promote retention.
Last, the legislation could also increase funding for HRSA Title VII workforce development programs.
Expand loan repayment programs to include more health workers, especially those who come from disadvantaged backgrounds and/or racial or ethnic minorities.
The Committee should consider legislation that would expand loan repayment programs that provide for student loan repayment in exchange for service commitments for a range of different types of health care providers.
The Committee could look to S. 462 (The Mental Health Professionals Workforce Shortage Loan Repayment Act of 202313) as a guiding example. This bipartisan legislation would address the current lack of incentives for mental health providers working in the Substance Abuse treatment to serve in areas that struggle to recruit and retain physicians. It would also create new incentives to attract providers to serve in underserved areas. This legislation would repay up to $250,000 in eligible student loan repayment for mental health professionals who work in mental health professional shortage areas.
The Committee should consider these policy ideas and extend them to additional provider types experiencing severe shortage issues.
The Committee should also consider legislation that would incentivize current and former National Health Service Corps (NHSC) participants (physicians, nurses, and dentists) to enroll in demonstration programs to support entities, including long-term care facilities and hospitals at risk of losing obstetric services, experiencing severe staffing shortages.
The variety of settings experiencing severe staffing shortages also warrants consideration for expanding the NHSC to other qualified health specialties, including certain mental health professionals and direct care workers.
Ensure broad eligibility for federal programs intended to increase providers in underserved areas.
The Committee should consider utilizing expansive eligibility language in legislation intended to increase providers in underserved areas.
For example, Section 403 of the MISSION Act of 201814 directs the VA to expand its existing medical residency program to underserved non-VA facilities. The Act provides an expansive definition of “covered facility” for the purpose of the program by listing specific provider types and including “[s]uch other health care facility as the Secretary considers appropriate for purposes of this section” as a catch-all.
Safety from Violence for Healthcare Employees (SAVE) Act (H.R. 7961), legislation that would protect caregivers from workplace violence.
The bill, introduced by Reps. Madeleine Dean (D-Pa.) and Larry Bucshon, MD, (R-Ind.), would provide legal penalties, similar to federal protections that exist for flight crews, for individuals who knowingly and intentionally assault or intimidate hospital employees. Increasing threats and acts of violence against health care workers have further burdened a workforce already under immense strain from shortages, burnout, and trauma related to the COVID-19 pandemic. While Congress and the Department of Justice have addressed violence against airline workers, they have not done the same for the health care workforce.
The Coalition appreciates the opportunity to provide these comments and looks forward to working with the HELP Committee to identify bipartisan solutions to remedy our nation’s health care workforce shortages and develop these ideas into legislation. If you have questions or seek any additional information, please contact Elizabeth Cullen at the Jewish Federations of North America at Elizabeth.Cullen@jewishfederations.org.
Sincerely,
American Academy of Family Physicians
American Dental Association American Dental Education Association
American Health Care Association
America’s Essential Hospitals
ANCOR
Associations for Clinicians for the Underserved
National Association of Counties (NACO)
National Council of Urban Indian Health
National Health Care for the Homeless Council
The Jewish Federations of North America
About the Partnership for Medicaid
NCUIH is a member of the Partnership for Medicaid, which is a nonpartisan, nationwide coalition of organizations representing clinicians, health care providers, safety-net health plans, and counties. The goal of the coalition is to preserve and improve the Medicaid program. Members of this coalition include:
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501Mary Jomiahttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngMary Jomia2023-03-20 10:25:582023-06-20 10:46:50NCUIH Joins Partnership for Medicaid in Letter to Senate on Addressing Healthcare Shortages
We need your help contacting Congress to support increased healthcare resources for urban Native communities.
Representatives Ruben Gallego (D-AZ-3) and Raúl Grijalva (D-AZ-7) are again leading a letter to the Chair and Ranking Member of the Appropriations Subcommittee on Interior, Environment, and Related Agencies. This subcommittee appropriates funding for the Indian Health Service (IHS) and Urban Indian Organizations (UIOs).
The letter requests an increase for the urban Indian health line item to $973.59 million for Fiscal Year 2024 and retaining appropriations for IHS. Adequate funding for urban Indian health is necessary to fulfill the federal government’s trust responsibility to all American Indians and Alaska Natives. The proposed amount is determined by the Tribal Budget Formulation Workgroup (TBFWG) as part of the request for full funding for IHS at $51.4 billion.
We encourage you to contact your Member of Congress and request that they sign the Gallego-Grijalva Urban Indian Health Letter by the deadline of March 17.
You can use the text below as a template to call and/or email to email your Member of Congress. You can find your representative here.
Sincerely,
The National Council of Urban Indian Health (NCUIH)
Step 3: Paste the email into the form and send. Please contact Lycia Maddocks (LMaddocks@ncuih.org) with questions.
Email to Your Member of Congress
Dear Representative,
As an urban Indian health advocate, I respectfully request you sign on to the Gallego-Grijalva letter to the Chair and Ranking Member of the Appropriations Subcommittee on Interior, Environment, and Related Agencies. The letter requests an increase for the urban Indian health line item to $973.59 million for Fiscal Year 2024 and retaining appropriations for IHS. Adequate funding for urban Indian health is necessary to fulfill the federal government’s trust responsibility to all American Indians and Alaska Natives. The proposed amount is determined by the Tribal Budget Formulation Workgroup (TBFWG) as part of the request for full funding for IHS at $51.4 billion.
It is the policy of the United States “to ensure the highest possible health status for Indians and urban Indians and to provide all resources necessary to effect that policy.” This requires that funding for Indian health must be significantly increased if the federal government is to finally fulfill its trust responsibility. At a minimum, funding must be maintained and protected as budget-cutting measures are being considered.
We respectfully ask that you join this year to help honor the federal trust obligation and support the overall health and well-being of American Indians and Alaska Natives.
To sign on to the letter, please contact Emma Reidy (Emma.Reidy@mail.house.gov) from Gallego’s office by this Friday, March 17.
Thank you for your leadership and commitment to upholding the United States’ trust and treaty responsibility.
https://ncuih.org/wp-content/uploads/Website-Graphics-Logo-Package_NCUIH_D081_V1_Policy-Update.png11261501LMaddockshttps://ncuih.org/wp-content/uploads/NCUIH-2022-Logos_Full-Logo-3.pngLMaddocks2023-03-17 11:01:082023-03-17 11:06:22UPDATED: Contact Congress to Increase Funding for Urban Indian Health TODAY
Yesterday, President Biden released the annual budget proposal for Fiscal Year (FY) 2024. The Budget proposes $9.7 billion for the Indian Health Service (IHS), an increase of $2.5 billion or 36% above FY23 enacted levels.
NCUIH CEO Francys Crevier testified before Congress, and Committee leaders pledged to protect the Indian Health Service budget from cuts.
Read on to learn more.
Biden Budget Proposal Demonstrates Continued Commitment to Improving the Indian Health Service
On March 9, 2023, the President released the annual budget proposal for Fiscal Year (FY) 2024. The “HHS Budget in Brief” has been released but the Congressional Justification for the Indian Health Service has not been released.
The bottom line: Mandatory Funding for IHS Remains a Priority; Advance Funding Still Needed
What they’re saying: “The Administration is committed to upholding the United States’ trust responsibility to tribal nations by addressing the historical underfunding of IHS. The enactment of an advance appropriation for 2024 for IHS was a historic and welcome step toward the goal of securing adequate and stable funding to improve the overall health status of American Indians and Alaska Natives.”
The budget proposal includes the Administration’s commitment that by 2025, the IHS budget would shift from mostly discretionary to all mandatory funding.
The President also reaffirmed that “until [mandatory funding] is enacted, it is critical that Congress continue to prioritize advance appropriations for IHS through the discretionary appropriations process to ensure funding for healthcare services and critical facilities activities are not disrupted.”
The big picture: NCUIH will continue to advocate for the Tribal Budget Formulation Workgroup requests for urban Indian health and the Indian Health Service.
What’s next: Congress will hold hearings to review the President’s request. House Republicans are calling for reduced spending levels, while Senate appropriators are having bipartisan talks on top-line totals, with a goal of starting spending bill markups as soon as May.
By the numbers:
This chart shows how the enacted amounts compare to the Tribal request and President proposals.
Overall Budget for Department of Health and Human Services (HHS)
The Budget requests $144 billion in discretionary budget authority for FY24, a $14.8 billion or 11.5% increase from the FY23 enacted level.
Indian Health Service Budget Highlights
Indian Health Service Overall: $9.7 billion, an increase of $2.5 billion or 36% above FY23 enacted and $41.7 billion less than requested by TBFWG.
Urban Indian Health:$115 Million for an increase of $25 million or 27% above FY23 enacted and $858.6 million less than requested by the TBFWG.
Reauthorizes and Increases Funding for the Special Diabetes Program for Indians: The budget proposes to reauthorize the Special Diabetes Program for Indians and provide $250 million in FY24, $260 million in FY25, and $270 million in FY26 in new mandatory funding.
Proposes New Program to Increase Public Health Capacity and Infrastructure: The budget also proposes new funding of $150 million in FY25 to address public health capacity and infrastructure needs in Indian Country. This funding would support an innovative hub-and-spoke model to address local public health needs in partnership with tribes and urban Indian organizations.
Bipartisan Pledge from House Committee Leaders to Protect Indian Health Service Budget from Budget Cuts
NCUIH CEO, Francys Crevier (Algonquin), testifies at American Indian and Alaska Native Public Witness Day.
On March 9, 2023, the National Council of Urban Indian Health CEO Francys Crevier (Algonquin), testified before the House Interior Appropriations Subcommittee as part of American Indian and Alaska Native (AI/AN) Public Witness Days regarding FY24 funding for the Indian Health Service. NCUIH was invited to testify on the critical health needs of American Indians and Alaska Natives living in urban areas.
Did you know?: It was the first hearing of this Subcommittee with the return of Chairman Mike Simpson.
NCUIH’s testimony called attention to the staggering health disparities that Native communities face and requested full funding for the Indian Health Service.
“Native people deserve full, healthy lives. We cannot continue to rely on short-term solutions that only address the symptoms of the problem. We ask for full funding for IHS and the urban Indian health line item. Make advance appropriations and 100% FMAP for UIOs permanent. Protect us from sequestration now.”
– Francys Crevier (Algonquin), NCUIH CEO
Following Ms. Crevier’s testimony, Chairman Simpson pledged to prioritize protecting the Indian health budget from the expected budget cuts.
“We are going to have to make sure that we prioritize Indian healthcare in these budgets…There are some areas we’re going to have to protect and Indian health is going to have to be one of them.”
-Chairman Mike Simpson (R-ID)
Ranking Member Chellie Pingree also attended and reaffirmed her continued commitment to prioritizing Native health care.
“Protecting Indian health is critically important, as is housing and education and so many other things, but meeting our treaty and trust obligations is just so critical… The idea that the budget is six, seven billion but should be 51, we just have to take a big leap at getting closer because you and the centers you represent know how to distribute and spend that money and know how to make sure we get access to it and that you can use it in the ways that its most important for [Tribes and Urban Indian Organizations].”
– Ranking Member Chellie Pingree (D-ME)
Our thought bubble: NCUIH applauds the bipartisan leadership of Chair and Ranking Member of the Appropriations Committee.