In this Edition:
- 📊 Government Shutdown Ended & FY 2025 Funding Extended
- 🤝 NCUIH at the 2025 NCAI Annual Convention & Marketplace
- 💻 NCUIH Comment Submission on IHS Health IT Modernization
- 🏷 NCUIH Requests UIO Exemption from HRSA’s 340B Rebate Model Pilot Program
- 🗓 IHS Tribal Consultation & Urban Confer on Agency Realignment
- 🩺 Updates from the IHS Tribal Leaders Diabetes Committee (TLDC)
- 💬 CMS Tribal Technical Advisory Group (TTAG) Meeting Highlights
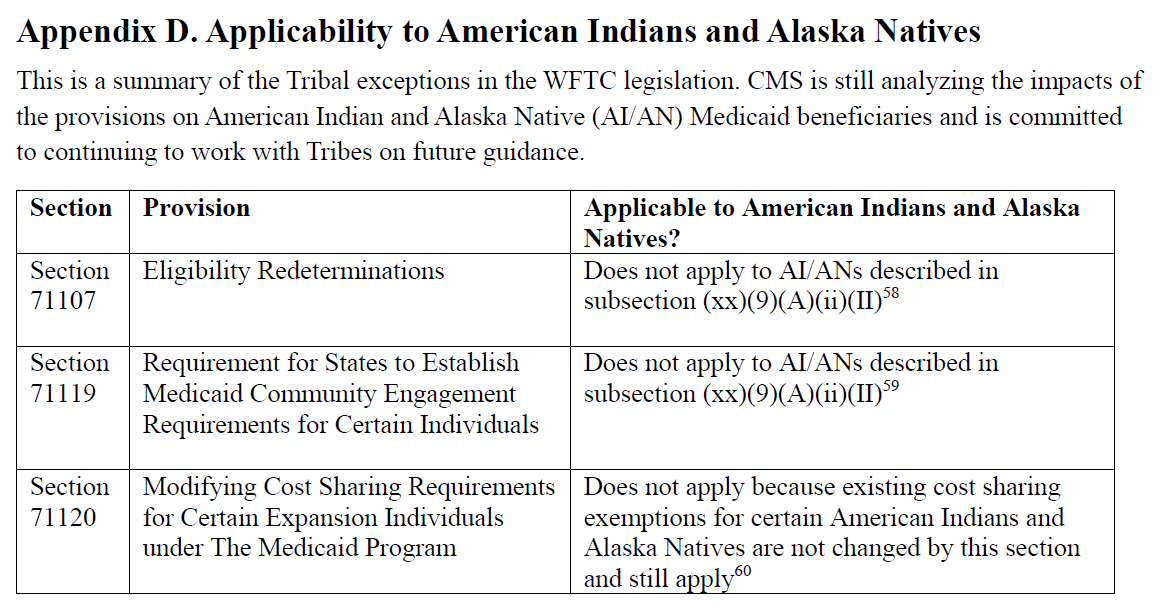
- 📘 CMS Guidance on AI/AN Exemptions in OBBBA Medicaid Work Requirements
- 📝 CMS Informational Bulletin on OBBBA Medicaid & CHIP Provisions
- 👥 Federal Hiring Freeze Lifted & IHS Staffing Updates
- 🎗 IHS Request for Urban Cancer Care Services Data for Mapping Initiative
- 📈 IHS FY 2028 Budget Formulation Updates
NEW: Strategy Guide Release — Strategy 1: Strengthening Health Care Access for Urban American Indian and Alaska Native People

This month, NCUIH released Strategy 1 of our new multi-part Strategy Guide series designed to support Urban Indian Organizations in delivering high-quality, culturally grounded health care. Building on our Investing in Wellness: Financing Strategies for Behavioral Health in Indian Country work, Strategy 1 outlines practical ways to strengthen Medicaid reimbursement for behavioral health services and expand sustainable financing options that support prevention, treatment, and recovery efforts at UIOs
Explore Strategy One Material and Resources for UIOs: Visit the NCUIH Website
Government Shutdown Ended, Government Funded through End of January
On November 12, Congress passed a spending package keeping FY 2025 funding through January 30, 2026.
• SDPI funded at $53.15 million through January.
• Enhanced ACA subsidies were not extended.
• The Continuing Resolution (CR) reversed all Reduction In Force (RIF) actions taken since October 1 and prevents further RIFs during the CR period.
→ Go Deeper: Link to NCUIH analysis.
NCUIH in Action

NCAI 2025 Annual Convention & Marketplace
NCUIH President Walter Murillo co-chaired the Health Subcommittee.
Health resolutions that passed included:
- UIO inclusion in Medicaid 1115 waivers
- 15% HHS Tribal set-aside
- Protecting IHS in Medicaid reforms
- Extending FEHB to Tribal retirees
- Safeguarding AI/ANs in OBBBA
- Codifying HHS Tribal advisory committees
- Preserving Medicaid reimbursement rates
- Supporting Native youth leadership in substance-abuse prevention
NCUIH also participated in:

- December 4 – Pharmaceutical Research and Manufacturers of America Annual Holiday Partner Celebration – Connecting with health sector partners and stakeholders.

- December 9- Partnership for Medicaid End-of-Year Meeting – Strengthening collaboration with coalition members and contributing to shared Medica55id policy priorities affecting Urban Indian Organizations.

- December 11 – NCUIH with Rep. Adelita Grijalva (AZ-07) at the House Natural Resources Subcommittee on Indian and Insular Affairs hearing on Modernizing the Implementation of 638 Contracting at the Indian Health Service.
NCUIH Comment Submission on Indian Health Service Health Information Technology Modernization
NCUIH Comment Submission on Indian Health Service Health Information Technology Modernization
- Background: NCUIH submitted comments requesting clarity on 24-hour technical support, functionalities of the Patients at the Heart electronic health record, documentation pathways for Traditional Healing, and continued engagement with Urban Indian Organizations.
- NCUIH recommended: Ongoing consultation and transparent implementation planning.
NCUIH Request for Urban Indian Organization Exemption from 340B Rebate Pilot
- Background: NCUIH submitted a formal letter requesting the Health Resources and Services Administration to exempt Urban Indian Organizations and Indian Health Care Providers from the proposed 340B Rebate Model Pilot due to financial and administrative burdens.
- NCUIH recommended: Full exemption for the Indian Health Service, Tribal, and Urban Indian health system.
Indian Health Service Agency Realignment Tribal Consultation and Urban Confer

February 9, 2026 — Indian Health Service Agency Realignment Tribal Consultation and Urban Confer
- Background: The Indian Health Service is gathering Tribal and Urban Indian Organization feedback on its proposed organizational realignment.
- What’s Next: Written comments are due February 9, 2026, and may be submitted through the Indian Health Service consultation portal or emailed to urbanconfer@ihs.gov.
UIO Important Dates:
- Urban Confer (virtual only): Thursday, January 15, 2026, 1:00 – 4:00 PM ET (rescheduled from Jan. 8)
- NCUIH will be holding a virtual prep session for UIOs on January 14, 2026, at 1pm ET.
Tribal Consultations
UIOs are invited to the Tribal Consultations in-person to listen.
- December 15, 2025, 1:00 – 4:00 PM CT (Durant, OK)
- December 16, 2025, 1:00 – 4:00 PM MT (Denver, CO)
- December 17, 2025, 1:00 – 4:00 PM PT (San Diego, CA)
- December 22, 2025, 2:00 – 5:00 PM ET (Virtual)
- January 5, 2026, 1:00 – 4:00 PM MST (Flagstaff, AZ)
- January 6, 2026, 1:00 – 4:00 PM PT (Seattle, WA)
- January 7, 2026, 1:00 – 4:00 PM MST (Billings, MT)
- January 8, 2026, 1:00 – 4:00 PM CST (Green Bay, WI)
Upcoming Events and Important Dates

IHS & Federal Agency Updates
IHS Tribal Leaders Diabetes Committee (TLDC) — Dec. 2
- SDPI FY 2026 funding: 6-month awards (Jan–June); remainder to be issued when Congress fully authorizes SDPI.
TLDC recommended:
– 25% administrative supplements to all SDPI recipients (2026–27)
– Sharing area-level unobligated balances
– SDPI data impact analysis
Centers for Medicare & Medicaid Services Informational Bulletin Update
CMS TTAG Meeting — Dec. 8
- Tribal guidance on OBBBA coming this winter.
- CMS DTA pursuing Tribal exemption for HRSA’s 340B Model Rebate Pilot.
- Ongoing vacancies: IHS Director and CMS DTA Director positions.
- CMS encourages Tribal–state engagement for RHTP implementation.

On November 18, the Centers for Medicare & Medicaid Services issued an informational bulletin clarifying how Medicaid and Children’s Health Insurance Program provisions in the One Big Beautiful Bill Act apply to American Indians and Alaska Natives. The bulletin confirms that eligibility redeterminations, Medicaid community engagement requirements, and modified cost-sharing provisions do not apply to eligible American Indian and Alaska Native individuals, including Urban Indians. Additional guidance issued on December 8 reiterates that American Indians and Alaska Natives are excluded from Medicaid work requirements.
Federal Hiring Freeze Ended — Oct. 15
- IHS is preparing staffing plans under the Continued Accountability in the Federal Government’s Employment Executive Order.
- Vacancies will begin to be filled once the plan approved.
IHS Staffing Updates
- Clayton Fulton now carries out duties of Acting IHS Director.
- Benjamin Smith returns to Deputy Director.
- Darrell LaRoche resumes Deputy Director for Management.
- Dr. Rose Weahkee returns to Associate Deputy Director for Management Operations.
IHS Health IT Modernization — NCUIH Comments Submitted
NCUIH requested:
• Clarification on 24-hour national helpdesk function
• Details on PATH EHR capabilities
• Support for Traditional Healing documentation
• Continuous engagement with UIOs throughout modernization
IHS Request for Urban Cancer Care Services Data
IHS FY 2028 Budget Formulation
• Tribal request: $29.8 billion mandatory funding for IHS
• January 21–22, 2026: Area report presentations
• February 10–11, 2026: National Budget Formulation Work Session
BADGES for Native Communities Act Update
- On December 12, 2025, the Bridging Agency Data Gaps and Ensuring Safety for Native Communities Act unanimously passed the United States Senate and now advances to the House of Representatives.
- The bipartisan legislation strengthens Tribal public safety, improves reporting on Missing or Murdered Indigenous Peoples, and establishes a grant program to support coordinated response efforts.
- Urban Indian Organizations are eligible entities under the grant program.
Reminder: One Big Beautiful Bill Act Resource for Urban Indian Organizations

NCUIH has developed a resource to help Urban Indian Organizations understand Medicaid and Children’s Health Insurance Program provisions under the One Big Beautiful Bill Act. The resource outlines which provisions apply to Urban Indian Organizations and clarifies protections and exemptions for American Indian and Alaska Native patients during state-level implementation.
UIO Input Request
NCUIH is continuing to engage with federal partners on several policy developments that may affect Urban Indian Organizations, including Indian Health Service (IHS) Realignment efforts and broader discussions related to care delivery and program administration.
To strengthen NCUIH’s advocacy and ensure UIO perspectives are accurately reflected,we invite UIOs to share feedback and experiences related to the following:
- IHS Realignment Participation: Are you planning to attend any upcoming in-person consultations related to IHS Realignment?
- Realignment Concerns: Do you have concerns or considerations regarding the proposed IHS Realignment, particularly as it relates to UIO operations or service delivery?
- Contract Centralization: How might the proposed centralization of contracts at IHS Headquarters, rather than through Area Offices, impact your organization? Are there specific concerns you would like NCUIH to elevate?
- Food is Medicine Programs: Do any UIOs currently operate or plan to develop Food is Medicine programs specifically designed to support cancer patients?
Feedback shared will help inform NCUIH’s ongoing policy engagement, written comments, and participation in consultations and advisory discussions.
How to respond: UIOs are encouraged to share feedback by emailing policy@ncuih.org.
Save the Date: 2026 NCUIH Annual Conference

Join us for our 2026 Annual Conference on April 27–30, 2026, at The Westin Downtown in Washington, D.C. The conference will bring together Urban Indian Organizations, health leaders, policymakers, and partners to share strategies, strengthen systems, and advance urban Indian health nationwide. Programming includes UIO board training, two full days of conference sessions, and a Hill Day for Urban Indian Organizations. NCUIH is also accepting session and poster proposals, with submissions due January 15, 2026.
One Last Thing — Check Out This Upcoming Funding Opportunity
Urban Indian Organizations can now apply for funding to support culturally grounded overdose prevention projects.
Applications are due January 16, 2026, with awards of up to $45,000.
Our partners at Seven Directions and the National Network of Public Health Institutes are sharing materials to help spread the word—please repost or use the linked graphics to share this opportunity with your community.
About NCUIH
The National Council of Urban Indian Health (NCUIH) is a national representative for the 41 Urban Indian Organizations contracting with the Indian Health Service under the Indian Health Care Improvement Act. NCUIH is devoted to the support and development of high quality and accessible health and public health services for American Indian and Alaska Native people living in urban areas.
NCUIH respects and supports Tribal sovereignty and the unique government-to-government relationship between our Tribal Nations and the United States. NCUIH works to support those federal laws, policies, and procedures that respect and uplift Tribal sovereignty and the government-to-government relationship. NCUIH does not support any federal law, policy, or procedure that infringes upon or in any way diminishes Tribal sovereignty or the government-to-government relationship.