On July 1, 2025, the Senate passed their budget reconciliation bill. The Senate’s One Big Beautiful Bill Act is a major bill that would deliver the significant elements of President Trump’s legislative agenda, including tax cuts, Medicaid reforms, and lifting the debt ceiling. The bill contains a health title, which includes Medicaid reform provisions, such as cost-sharing and provider tax changes. The Senate bill has notable provisions impacting American Indian and Alaska Native healthcare compared to the House-passed bill: exempts American Indian and Alaska Native beneficiaries, including “Urban Indians”, from the Medicaid and Supplemental Nutrition Assistance Program (SNAP) community engagement requirements and exempts American Indian and Alaska Native beneficiaries from more frequent eligibility redetermination requirements.
NCUIH Action
The National Council of Urban Indian Health (NCUIH) has worked with Urban Indian Organization (UIO) leaders and national partners, including the National Indian Health Board, and the National Congress of American Indians, and the Coalition for Tribal Sovereignty to ensure that American Indian and Alaska Native Medicaid and SNAP beneficiaries are protected from harmful policy changes.
Next Steps
The bill will return to the House to be voted on, and its passage remains unclear. There is a stated deadline of July 4.
Analysis
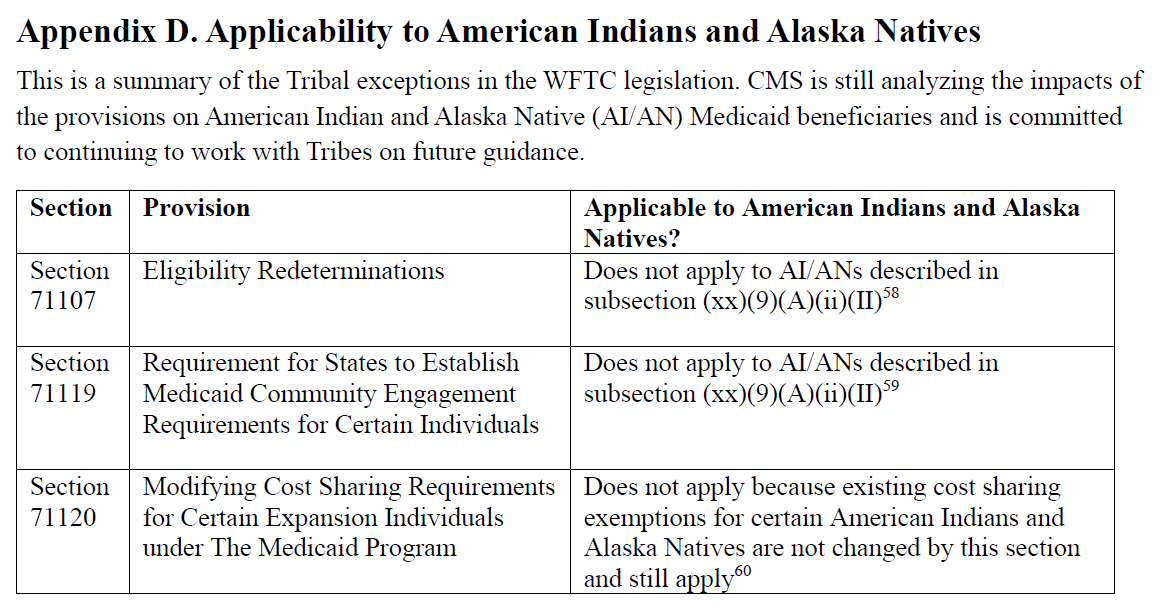
Community Engagement Requirements for Certain Medicaid Beneficiaries
What it Does: States would be required to implement community engagement requirements for able-bodied adults without dependents. Compliance may be achieved through:
- Working, volunteering, or participating in a work program for at least 80 hours/month; or
- Enrolling in educational programs totaling 80 hours/month.
Impact on Indian Country: The bill exempts American Indian and Alaska Native beneficiaries from these requirements. Specifically, it states that “specified excluded individuals” include:
- Indians and Urban Indians as defined in the Indian Health Care Improvement Act (IHCIA);
- California Indians as described in Section 809(a) of the IHCIA;
- Individuals determined eligible as an Indian for the Indian Health Service under regulations promulgated by the Secretary.
The work requirements go into effect on December 31, 2026.
Modifying Cost Sharing Requirements for Certain Expansion Individuals Under the Medicaid Program
What it Does:Requires states to impose cost sharing on Medicaid Expansion adults with incomes 100 – 138 percent of the federal poverty level (FPL). This cost-sharing is capped at:
- $35 per service.
- May not exceed five percent of the individual’s income.
Impact on Indian Country:American Indian and Alaska Native beneficiaries are already exempted from cost-sharing provisions for those who receive a “service directly by the Indian Health Service, an Indian Tribe, Tribal Organization, or Urban Indian Organization or through referral under contract health services for which payment may be made under this subchapter.” This exemption will remain in place.
Moratorium on New or Increased Provider Taxes
What it does: Reduces the safe harbor limit for states that have adopted the Affordable Care Act (ACA) expansion by 0.5% annually starting in fiscal year 2028 until the safe harbor limit reaches 3.5% in FY 2032.
Potential Impact on Urban Indian Organizations: UIOs are exempt from provider taxes due to their tax status and will not be affected by this provision.
Reduction in Expansion FMAP for States Covering Undocumented Immigrants
What it Does:Reduces by 10% the Federal Medical Assistance Percentage (FMAP) for Medicaid Expansion States who use their Medicaid infrastructure to provide health care coverage for undocumented immigrants under Medicaid or another state-based program.
Impact on States with Urban Indian Organizations: Seven states currently provide such coverage: California, Washington, Oregon, Minnesota, Illinois, New York, and Colorado, all of which have UIOs. States will have to individually decide on how and if they will adapt their programs to adjust to the potential decrease in federal funding. Several states, including California, Minnesota, and Illinois, have announced plans to freeze or cut these programs.
Modifications to SNAP Work Requirements for Able-Bodied Adults
What it does: Instituting exceptions to the SNAP work requirements for able-bodied adults.
Impact on Indian Country: The bill exempts American Indian and Alaska Native beneficiaries from these requirements. Specifically, it states that “specified excluded individuals” include:
- Indians and Urban Indians as defined in the Indian Health Care Improvement Act (IHCIA);
- California Indians as described in Section 809(a) of the IHCIA.
Medicaid Redetermination Period
What it does: Requires states to conduct eligibility redeterminations at least every 6 months for Medicaid expansion adults beginning after December 31, 2026. It also requires the Secretary of Health and Human Services to issue guidance within 180 days of enactment.
Impact on Indian Country: The bill exempts American Indian and Alaska Native beneficiaries from these requirements. Specifically, it states that “specified excluded individuals” include:
- Indians and Urban Indians as defined in the Indian Health Care Improvement Act (IHCIA);
- California Indians as described in Section 809(a) of the IHCIA;
- Individuals determined eligible as an Indian for the Indian Health Service under regulations promulgated by the Secretary.