Congress Approves Final Six Spending Bills for FY 2024, Includes Funding for Native Cancer Initiative and UIO Behavioral Health Project Funding
The bill includes $116.8 billion for HHS—a $995 million increase, and $6 million for new Improving Native American Cancer Outcomes Initiative.
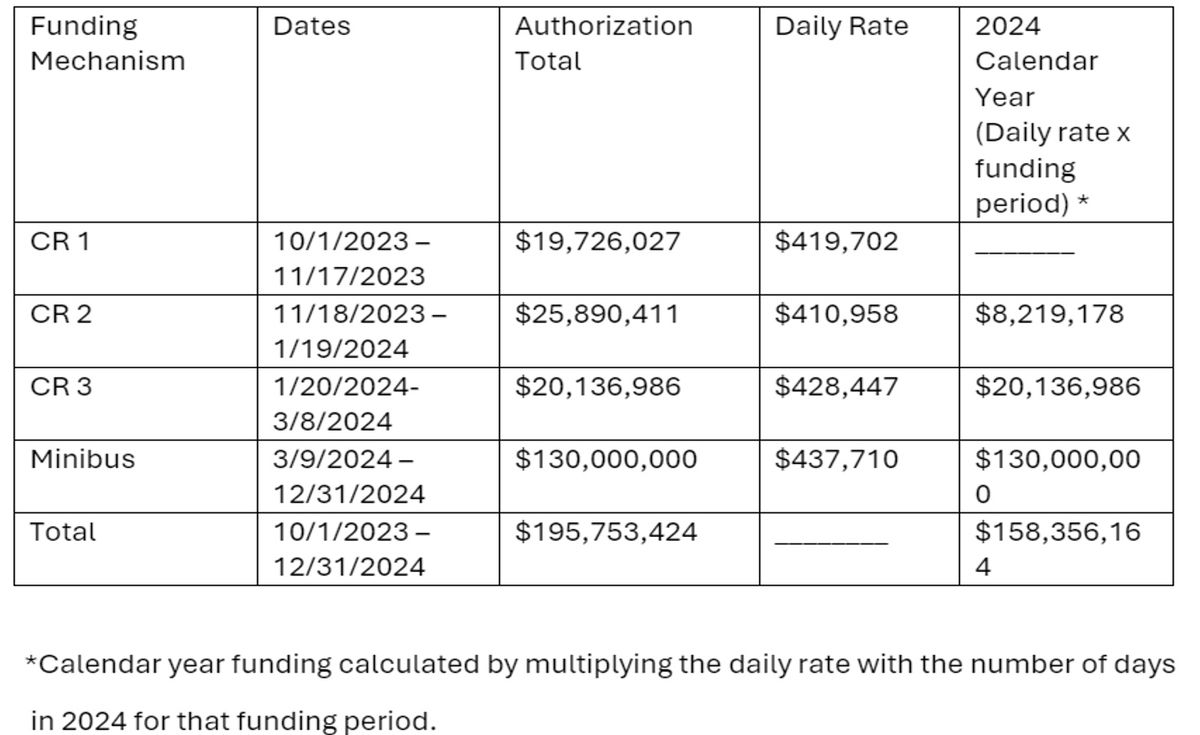
On March 23, 2024, the Further Consolidated Appropriations Act, 2024 (H.R.2882), also known as a ‘minibus,’ was signed into law by President Biden, finalizing appropriations for the remaining six spending accounts for fiscal year (FY) 2024. This follows the passage of the Consolidated Appropriations Act, 2024 on March 8, that finalized the first six spending accounts, including the Interior appropriations bill. The bill, which passed in the House with a 286-134 vote, followed by final passage in the Senate with a 72-24 vote, is the final package of final spending bills for FY 2024 and included Labor, Health, and Human Services (LHHS) appropriations.
The minibus appropriates $116.8 billion for the Department of Health and Human Services (HHS) for FY 2024, which is $995 million above the comparable FY 2023 level; $7.4 billion for Substance Abuse and Mental Health Services Administration (SAMHSA) for FY 2024, which is $19 million above the FY 2023 enacted level; and $8.9 billion for Health Resources and Services Administration (HRSA), an increase of $54 million compared to FY 2023 enacted levels. Despite tight budget constraints, there were modest increases and protection of current funding levels for key programs in HHS.
UIOs Included in Improving Native American Cancer Outcomes Initiative
The LHHS spending bill appropriates $6 million to Improving Native American Cancer Outcomes, which creates the Initiative for Improving Native American Cancer Outcomes. The bill directs the National Institute on Minority Health and Health Disparities to locate the Initiative at an NCI-designated cancer center demonstrating strong partnerships with Tribes, Tribal Organizations, and urban Indian organizations, to ultimately improve the screenings, diagnosis, and treatment of cancer for Native patients. NCUIH was proud to successfully advocate for the inclusion of UIOs in this critical program for all Native communities.
Protection of HIV/AIDS Funding
Congress successfully protected funding for HIV/AIDS prevention and treatment. The LHHS bill protected critical funding sources for key programs that work to improve health outcomes for Native communities, such as $2.6 billion for the Ryan White HIV/AIDS program, $165 million for Ending the HIV Epidemic, and $60 million for the Minority HIV/AIDS Prevention and Treatment Program, which includes a $5 million Tribal set-aside. Despite threats to cut funding to this vital program, Congress was ultimately able to save the Ryan White HIV/AIDS program, saving thousands of lives across the country. This program provides grants to eligible entities, including UIOs, to aid in the prevention and treatment of HIV/AIDS.
Native H.E.A.L. Program Funding Secured
The Labor, Health, and Human Services bill also provided Native American Lifelines of Boston Community Project Funding to create the Native H.E.A.L. program. This funding will allow Native American Lifelines of Boston (NAL) to engage in activities focused on the behavioral health needs of Urban American Indians in Massachusetts by providing culturally informed education on opiates, medication-assisted treatment (MAT), harm reduction strategies and/or risk factors related to opiate use disorder. Senator Warren and Senator Markey are strong supporters of NAL Boston and were critical in securing this Community Project Funding NAL Boston.
Bill Text:
- Full Legislative Text, Consolidated Appropriations Act, 2024
- Explanatory Statement: Division D – Labor, Health and Human Services Appropriations Act, 2024
Overview of Labor, Health, and Human Services Funding:
Table
| Line Item | FY 2023 Enacted | FY 2024 President’s Budget Request | FY 2024 House Passed | FY 2024 Senate Passed | FY 2024 Enacted |
| Health Resources and Services Administration | $9.7 billion | $9.47 billion | $7.5 billion | $9.14 billion | $8.9 billion |
| Substance Abuse and Mental Health Services Administration | $7.5 billion | $10.6 billion | $7.28 billion | $7.7 billion | $7.4 billion |
| National Institute of Health | $47.5 billion | $50.77 billion | $45.12 billion | $49.2 billion | $48.6 billion |
| Centers for Disease Control | $9.2 billion | $11.64 billion | $7.59 billion | $7.77 billion | $9.2 billion |
Analysis:
Health Resources and Services Administration
- $8.9 billion for HRSA for FY 2024
- $2.6 billion for the Ryan White HIV/AIDS program for FY 2024
- $165 million for Ending the HIV Epidemic
- $365 million for Rural Health Programs
- $27 million for Native Hawaiian Health Care
- $128.6 million for National Health Service Corps
- $1 million for Center of Excellence for Eating Disorders – Screening and Referrals
Centers for Disease Control and Prevention
- $24 million for Good Health and Wellness in Indian Country for FY 2024
Office of the Secretary – General Departmental Management
- $60 million for the Minority HIV/AIDS Prevention and Treatment Program
- $5 million Tribal set-aside within the Minority HIV/AIDS Prevention and Treatment program
Substance Abuse and Mental Health Services Administration
- $7.4 billion for SAMHSA for FY 2024
- $4.2 billion for Substance Use Services for FY 2024
- $237 million for Substance Abuse Prevention Services
- $986.5 million for Mental Health Block Grant for FY 2024
- $520 million for 988 Implementation and Behavioral Health Crisis Services
- $130 million for Childrens Mental Health Services
- $1.93 billion for Substance Use Prevention, Treatment, and Recovery Service Block Grants
- $1.58 billion for State Opioid Response Grants
- $23.67 million for Tribal Behavioral Health Grants
National Institute on Minority Health and Health Disparities
- $6 million for Improving Native American Cancer Outcomes
- $4 million for a Native Hawaiian/Pacific Islander Health Research Office
Important Behavioral and Mental Health Provisions (Restoring Hope For Mental Health And Wellbeing)
- $14.5 million for grants for Tribes and Tribal Organizations for Medication-Assisted Treatment for Prescription Drug and Opioid Addiction
- $14 million for Peer-Supported Mental Health Services
- $15 million for Infant and Early Childhood Mental Health