Urban Indian Health Policy Updates
NCUIH has been busy: this year we have already submitted 18 comments to federal agencies in 2022. To compare, we submitted 22 in 2021!
NCUIH Honors 2022 Urban Indian Health Champions
Yesterday, NCUIH celebrated 2022 honorees: Libby Washburn, Senators Padilla and Moran, along with Representatives Leger Fernandez and Joyce.
On May 24, 2022, the National Council of Urban Indian Health awarded four Congressional Urban Indian Health Champion Awards and one Award for Advocacy and Leadership in Urban Indian Health.
- The Congressional Urban Indian Health Champion Awards were given to four members of Congress for their outstanding advocacy on behalf of urban Indian health: Senator Alex Padilla (D-CA), Senator Jerry Moran (R-KS), Representative Teresa Leger Fernandez (D-NM-03), and Representative David Joyce (R-OH-14). Libby Washburn (Chickasaw Nation of Oklahoma), the former Special Assistant to the President for Native Affairs, was awarded the Advocacy and Leadership in Urban Indian Health award.
- What they’re saying: “The federal government must honor our country’s responsibility to Tribal Nations and urban Indians in all our policy decisions. Urban Indian organizations are a lifeline to Native Americans living in urban areas across California and across the nation and yet too many facilities are aging and underfunded,” said Senator Padilla.
- Last year, NCUIH recognized Senator James Lankford (R-OK), Senator Tina Smith (D-MN), the late Representative Don Young (R-AK-AL), and Representative Ruben Gallego (D-AZ-7) as the 2021 Urban Indian Health Congressional Champions.
NCUIH thanks the awardees for their dedication to upholding the federal trust and treaty obligation to provide the highest level of health to all American Indians/Alaska Natives.
Go deeper: https://ncuih.org/2022/05/25/press-releasencuih-honors-2022-urban-indian-health-champions/
New Resource: Urban Indian Health Funding

Despite the trust and treaty obligation of the federal government to provide health care to AI/ANs, urban Indian health has been historically underfunded and insufficient to meet the needs of AI/ANs living in urban areas.
NCUIH recently released a one-pager showcasing the history of funding for the urban Indian health line item of the Indian Health Service (IHS) budget.
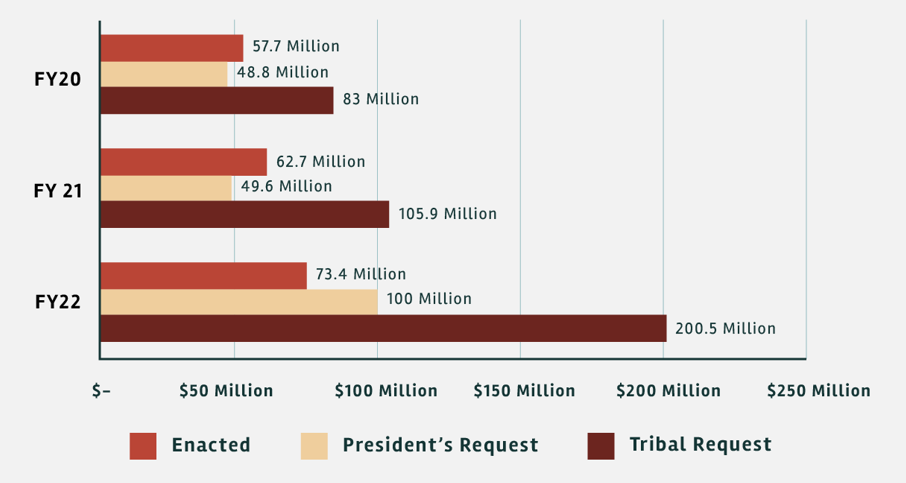
- This document shows a graph of the Tribal Budget Formulation Workgroup Request, President’s Budget Request, and enacted funding amounts for urban Indian health for fiscal years 2020, 2021, and 2022.
- Unfortunately, year after year, the Tribal Budget requests have gone largely ignored as evidenced in this resource.
- The graphs are intended to convey how far we need to go to begin meeting the health care needs of all American Indians/Alaska Natives (AI/AN).
- The bottom line: Urban Indian organizations (UIOs) provide a range of services for the urban AI/AN population and receive only about 1% of the total IHS annual budget.
By the numbers: The FY 2022 urban Indian health line item is currently just $73.4 million, which represents a 17.13% increase above the FY 2021 enacted level and the highest increase in the past 10 years. This amount, however, is insufficient and falls well below the Tribal Request of $200.5 million.
NCUIH Submits Comments to DOJ on Missing and Murdered Indigenous People

On April 15, 2022, NCUIH submitted written comments and recommendations in response to the Department of Justice’s (DOJ) Dear Tribal Leader letter seeking stakeholder input on the DOJ’s efforts to address the unacceptably high rates of violent crime in American Indian and Alaska Native communities and the missing and murdered Indigenous persons (MMIP) crisis. NCUIH thanked the DOJ for its commitment to working with Tribes to develop and support Tribally-driven solutions to violent crime and MMIP. NCUIH emphasized that working with all AI/AN communities across the United States is required by both Executive Order 14053, Executive Order on Improving Public Safety and Criminal Justice for Native Americans and Addressing the Crisis of Missing or Murdered Indigenous People (E.O. 14053). NCUIH further offered to assist DOJ in establishing strong working relationships with UIOs as it works to address these pressing public safety issues.
Bipartisan Group of Over Two Dozen Congressional Leaders Request Increased Resources for Urban Indian Health and Support Mandatory Funding

On April 26, 2022, Reps. Grijalva and Gallego along with 26 Congressional leaders requested up to $949.9 million for urban Indian health in FY23 and advanced appropriations for the Indian Health Service (IHS) until such time that authorizers move IHS to mandatory spending.
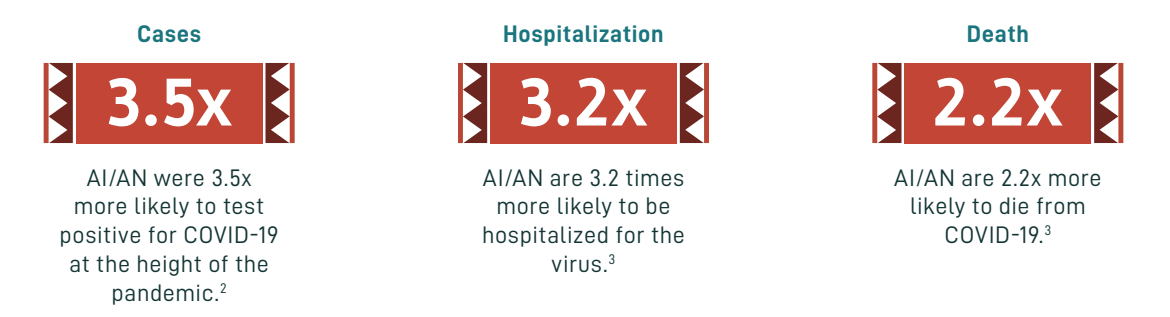
What they’re saying: The letter stated that “this increase in funding is necessary to address health disparities in the American Indian and Alaska Native (AI/AN) population. AI/ANs are 3.2 times more likely to be hospitalized for COVID-19 and 2.2 times more likely to die from the virus when compared with white patients.”
Why it matters: This letter comes as a continued effort by the NCUIH to address acute health disparities for AI/ANs living in urban areas. Congress has acknowledged these significant health care disparities in Indian Country.
Mandatory Funding: The Congressional leaders also stated their support for the President’s proposal of mandatory funding.
- The Indian health system is not shielded from the negative impacts of government shutdowns, continuing resolutions, and automatic sequestration cuts.
- Already underfunded, these disruptions can have serious consequences to UIOs’ ability to provide critical patient services.
- The letter states that “until authorizers act to move IHS to mandatory funding, we request that your subcommittee provide advance appropriations to the Indian health system to improve certainty and stability.”
The bottom line: This letter sends a powerful message to Chairwoman Pingree, Ranking Member Joyce, and members of Congress. In order to fulfill the federal government’s trust responsibility to all AI/ANs, funding for urban Indian health must be significantly increased.